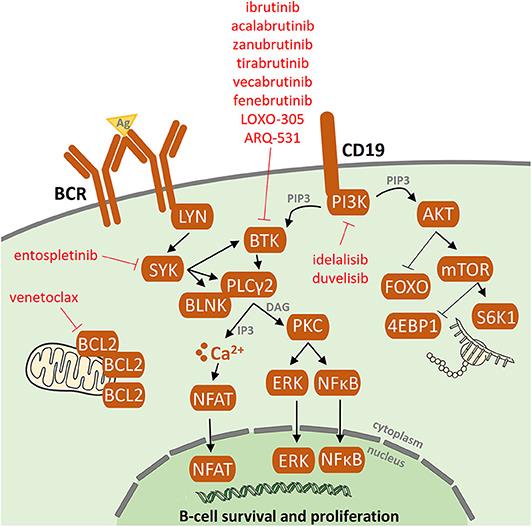
This is slightly complex but good overview of the acquired resistance mechanisms to novel agents.
In 80% of patients with ibrutinib failure, acquired mutations in BTK and PLCG2 genes were detected. No common resistance-associated mutations or deregulated signaling pathways have been reported in idelalisib failure. Acquired mutations in the BCL2 gene were detected in patients who had failed on venetoclax.
For 20% of patients, the ibrutinib resistance-associated mutations remain unknown. This data further supports the presence of alternative mechanisms of drug resistance other than BTK/PLCG2 mutations. To date, several candidate loci/mutations that may contribute to resistance have been described. These include del(8p) and SF3B1, PCLO, EP300, MLL2, and EIF2A mutations but these are only generally tested for in a research setting.
Resistance-associated mutations tend to occur between the second and fourth years of treatment and may be detected several months before clinical relapse.
They also discuss the development of next-generation agents for CLL patients who have acquired resistant mutations to current inhibitors.
I don't understand what kind of mutations this means? It seems to me that taking these inhibitors eventually leads to worse cll. Like its waking it up. I might be wrong but thats what I understood. Please correct me if in wrong.
Sushi, btk is an enzyme that there is too much of on cll cells which keeps the cll cells alive. Drugs like ibrutinib inhibit btk, allowing the cll cells to die as they are supposed to do.
There is a pathway through the btk enzyme to the cell nucleus. They have found that certain mutations to the btk enzyme and other enzymes in the pathway can lead to ibrutinib not being effective, that's known as resistance.
Particularly for those people starting out on ibrutinib, resistance like this is not common. The vast majority of people starting out on ibrutinib do very well. They think some of these mutations in the few people that have them may have been there even before they started taking ibrutinib.
There are a number of strategies for those that develop resistance. They can try new and different inhibitors like venetoclax that work on different pathways. And they have similar drugs to ibrutinib that may overcome resistance.
People who have multiple types of cll treatment can still do very well on ibrutinib, although they are more likely to have resistance than someone just starting out on ibrutinib.
There are many other drugs in development looking at other pathways, such that anyone starting out treatment today for cll can expect their cll will be under control for a very long time, if not indefinitely.
Interestingly, I asked Dr Wierda if I was to be tested for the mutations at ibrutinib onset and he said that he had never seen those mutations in patients pre ibrutinib.
I think what he said is true, but I also think they suspect, as Jackie writes, that there was some small subclone that grows due to selective pressure.
That would explain why you see btk mutations arise much more often in relapsed cll than in treatment naive cll.
One of the two founders of the CLL Society had an article on the fact that multiple studies show that ibrutinib and rituximab, in combination, is NO MORE EFFECTIVE than ibrutinib by itself. So, I've opted just for ibrutinib.
a little further info on this question of whether rituximab added to ibrutinib confers any benefit over ibrutinib alone...
The notion that rituximab adds no benefit to ibrutinib came out in 2018 as a result of the trials of ibrutinib vs. BR (Bendamustine+Rituximab). The study found that Progression-Free Survival after 2 years was:
However, it may be important to note that none of the patients in that study had been treated before. It is possible that rituximab added to ibrutinib might confer some benefit over ibrutinib alone in patients who are coming back for a second or third treatment. A clinical trial is being run right now to try to determine that:
Assuming this is your first treatment, then I think that's totally true - no benefit to adding rituximab to ibrutinib for patients who have never been treated before.
Four months. Started about April 1st. Was tolerating it quite well until a couple of weeks ago, but have since had increasingly severe reactions. Two days ago I unilaterally cut my 280mg dose in half—I had asked for 280 instead of 420 because I was afraid of adverse reactions—while yesterday I stopped taking all my vitamins. Along with drinking perhaps a gallon of water a day and getting a good night's sleep last night—thanks to my primary physician prescribing 10mg of Valium—I've had a wonderful day today as we near midnight on the east coast of the US. May you feel as well as I feel today!
Glad to hear you have had a great day! I read your note about Quercetin being a CYP3a4 inhibitor. I discovered that too. I got all set up with Quercetin on recommendation of a naturopath specializing in oncology.. But then read up on Quercetin and realized it has a cyp3a4 interaction. and that would not work with ibrutinib, which i was on at the time. So I have never taken it. And yes, lots of water very important and can make a big difference on lessening side effects.
I went through most of my 2.5 years of ibrutinib at just 140 mg. And it work very well while my weight was below 120 lbs. But when my weight rebounded to 132 lbs as my health recovered, my CLL started progressing ever so slightly. I had risen above the 2.5 mg per kg body weight formula for calculating minimum therapuetic dose of ibrutinib. So i increased the ibrutinib to 280 mg which held the CLL in check, but I got more arrhythmia/afib problems at the higher ibrutinib dose. So was ultimately switched to venetoclax.
Glad you had a naturopath. 99% of us have to find out things the hard way—unless one has an angel ion. their shoulders, like AussieNeil!!! An away, I'm sorry to hear about your fib. My wife had tachycardia for years, and finally got it resolved when she became one of the first patients to have an ablation. *** How are you doing on venetoclax? What dose? Any side effects? Did you have any withdrawal symptoms from stopping Ibrutinib? I'm concerned about the withdrawal symptoms from one, followed by adverse affects from the other. * P.S. When I spoke with my oncologist he advised against Calquest/acalabrutinib, because he said the side effects can be worse than those on Ibrutinib. Peace, love, and good health to you.
I do feel I had ibrutinib withdrawal when I stopped it and switched to venetoclax (even though the 2 drugs were overlapped for 4 weeks.
Venetoclax is great. I am having some digestive bowel problems - some queasiness after taking the pills, some bloat after eating, and occasional diarrhea. I think these are manageable and will reduce over time.
But each time I have tried to stay at the 400 mg dose of venetoclax, these problems have been too extreme. So I am back at 300 mg for now.
Re: Calquence/acalabrutinib - more than one person has said they hjad more side effects on Calquence than on ibrutinib. I know of people who went back to ibrutinib after trying Calquence. Including one person who had afib on ibrutinib - she also had it on Calquence. But it's very individual. For some people I suspect Calquence will be better.
I started on 280mg on Ibrutinib precisely because I was afraid of side effects, and I think that was one of the best decisions of my life. I recognize that the adverse effects I had were likely seriously magnified by certain vitamins and/or supplements being potent inducers; however, the long and short of it is that not knowing in advance what one takes and how it may interact, I think it's always a wise decision to start any drug at a lower dose and move up, if well tolerated. Good luck on your venetoclax.
Hi thanks for the information, so I have mutation SF3B1 after initial diagnosis September 2018, so would i better not to have ibitrunib as a first line treatment or will it be the same for all treatments? It's so complex 😫
Heather, it's very complex and the article says only that it MAY contribute. There are many more variables and probably some we don't yet know about that may influence anyone's chances of developing resistance to any treatment.
Please don't get too focused on your SF3B1 mutation which is a sub clonal mutation. So, not all the CLL cells are affected but evidence suggests that the SF3B1 mutation might be linked to more aggressive and unpredictable disease. There is very little data though and none related to the new treatments.
There is a strong association with the 11q del subtype of CLL, which generally has an unmutated IGHV and shares the same prognostic features.
However, the vast majority of 11qdel and unmutated patients do very well on the new targeted treatments, including Ibrutinib and, at the moment, there is no evidence that the SF3B1 patients do worse than 11qdel and unmutated without SF3B1.
On a positive note SF3B1 mutation does not confer the same degree of poor prognosis as TP53 mutation or 17p deletion.
When you need treatment I would suggest looking for a clinical trial of targeted treatments rather than FCR as FCR will almost certainly not give you long term control of your CLL.
Thank you Jackie, I am approaching treatment as my lymphocytes have more than doubled in 6 months so want to look into this topic more in depth, my haematologist has said it wouldn't be FCR
My conclusion to the conclusion is - " We need to further study and observe resistance mutations and then develop testing to identify and overcome theses aberrations". Easy stuff.
Whatever the cocktail; I hope that it tastes good, costs less, and makes me feel skinny.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.