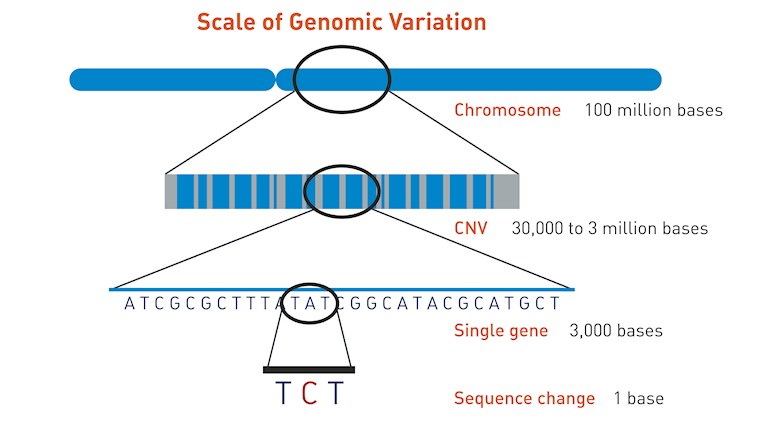
Chromosomal microarray (CMA) is clever, very sensitive technology which looks for extra (duplicated) or missing (deleted) chromosomal segments, sometimes called copy number variants (CNVs) - see illustration. These include: microdeletions and microduplications of chromosome segments, which are too small to see under a microscope but may contain multiple genes, most abnormalities of chromosome number (trisomy, monosomy, etc.) and most unbalanced rearrangements of chromosome structure (translocations, etc.)
CMA testing is often used to help the families of children with previously undiagnosed conditions but now it's also being used to establish clonality and high risk features in patients with Richter Transformation where it's helpful in tracking duplications or deletions of chromosomal segments, including aberrations involving TP53 and CDKN2A (a key regulator of cell cycle progression), which are known to be markers of poor prognosis.
This poster from ASH 2019 looks at 24 patients with a diagnosis of Richter transformation to DLBCL with a prior history of CLL/SLL. Of these patients, 7 had CMA performed on both the CLL/SLL and RT samples.
CMA was able to provide proof of common clonality in 6 of 7 patients with Richter transformation to DLBCL, which is a poor prognostic feature of RT. It also identified a loss of TP53 and/or CDKN2A in 5 of 7 patients, also a poor prognostic feature of RT.
"This information can be used to counsel patients on prognosis and could effect clinical recommendations such as treatment with allogeneic stem cell transplantation. Institutions with the ability to run CMA should utilize this modality in patients Richter transformation to DLBCL."
Jim have you ever come across any research on the affect of small sub clones in CLL that was previously untreated? I've been in w&w for 10 years with a large biallec deletion of 13q mutated. Recent repeat FISH showed 6 percent tp53. Trying to figure out what this might mean for me - apparently uncommon in untreated CLL, but I have had the disease for 10 years. Many thanks for any input!!
I wrote a post on the significance of small numbers of TP53 mutated clones and I think the answer was that it was an adverse prognostic factor at any level but did not affect the time to first treatment.
I am trying to find some information on the loss of CDKN2A at 9p21 along with a bunch of other copy number changes- currently untreated? can you shed any light on this?
Hi Elkk, I've had a look at your previous post with the results and the evidence for various prognostic factors. Remember, I'm not a doctor and I'm just looking at the published information. Your doctors will be able to interpret your results better, taking into account all the information they have and your clinical situation.
You appear to have a complex karyotype from your multiple deletions including the CDKN2A gene at 9p21. Loss of CDKN2A/B is a sparsely described in CLL although homozygous deletion (you have 70% loss) has recently been associated with resistance to venetoclax treatment. CDKN2A/B role in CLL progression via the signaling network around MYC is poorly understood but the CDKN2A/B gene area controls the cell-cycle regulators involved in slowing down cell proliferation at multiple levels so that reduced CDKN2A expression in combination with increased MYC expression can result in accelerated proliferation.
Loss of all CDKN2A/B has been directly associated with Richter transformation (RT) but del(9)(p21) had previously only observed in lymph node biopsies with histologically confirmed RT and not in corresponding peripheral blood samples acquired during the CLL phase.
You have a had quite a sophisticated investigation here but I can't see any results for TP53 mutation, del17p or a direct IGHV mutation test.
Complex karyotype and the loss of CDKN2A/B can be associated with a higher risk of chronic lymphocytic leukaemia likely to transform but ideally you need to be tested for mutations of NOTCH1 and MYC too in order to assess the full risk.
Remember that the information I've given you here is based on some research on various patient populations so it is statistical and that statistics tell you very little about what will happen to an individual person. Nothing is absolute and certain here.
I'm not sure I've been any help Elkk but I would be interested to know what your doctor says about the results you've shared and if they are going to test you for the other deletions and mutations.
Having another read of the report it states that it did NOT detect copy number changes in MYB(6q23), ATM (11q22.3),13q14 or TP53(17p13.1) and did NOT detect rearrangement 14q32.
I cannot see anything about MYC ,NOTCH 1 or IGHV..
Not sure if there is any significance of any of the other copy number changes?
Previous flow has said positive for cd38 but did not state a percentage.
You have been very helpful, I am very appreciative.
Elkk, apologies - I missed the TP53 on the report and the rest of my reply really focussed on the loss of CDKN2A. If the flow said positive for CD38 then it will have been over a set threshold ol percentage to consider it positive.
Take care and let us know if there is anything else
Hi Jackie, no apology needed, it was in fact my error, I had not included that paragraph. Would it be assumed that the cd38 was over the threshold to be used as a surrogate marker for IGHV? (unmutated?)
Although I thought I had a reasonable understanding of all this it seems that I am getting more confused the more complex this becomes! I think I need to go back to CLL grade school, I appreciate you sharing your vast knowledge, I do find that the more informed I am the less stress I have.
Yes, that's right Elkk, the cd38 will have been over the threshold to be used as a surrogate mutation status and you are likely to be unmutated. However, it's only a surrogate and you need a proper test.
It is hugely complicated and what might be true for one person is not true for another because of another set of variables!
You have been so helpful, just trying to be as informed as possible, it would be no surprise if I am in fact unmated, as I am heading to treatment soon after just over two years of W&W with lymphocytes doubling six monthly plus some other B Symptoms, it will be FCR as that is what is available first line here.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.