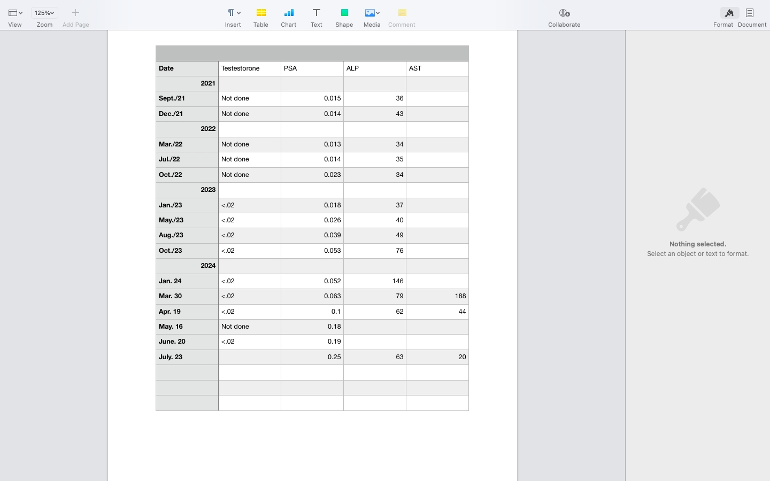
My PSA has been going up steadily for a couple of years. In Jan. of this year it was 0.052 and now is 0.25. It went up 25% in the last month. I am on Lupron and Abi. Seems like they are failing. I know, it is still low, but I am looking at my next options. I am not one to prolong life at any cost. I have an appt with my MO in a month as well as another PSA test.
I'm not a fan of chemo. It seems to only give an extra few months and the side effects are not great. My mets are in my bones so RAD 223 may be possible.
Asking for advice, as well as comments from you who have been through chemo and/or RAD 223.
Written by
gsun
To view profiles and participate in discussions please or .
Hello, Here is my experience. When I went to my MO @ dx, he laid out a path of treatment. (It was right before triplet therapy.) At the time I was on Lupron and Casodex (Started by my urologist.). He said if I do chemo early, he thought that I would have some years to live, not just months. He did not know how many. I have extensive bone Mets. I started chemo the end of Aug 2021. It will be 3 years this August. It wasn't all fun. But I am glad that I did it. . You can see detail in my profile. I did not do RAD 223--I have no clue. My Urologist thought that I should start with RAD-223. But MO did not. Again, just my experience
Greetings from the Whack! Although your PSA is still very low, when the Androgen Receptor Pathway Inhibitor (ARPI) drugs like Xtandi (enzalutamide) and Zytiga (abiraterone) start to fail you need to move to drugs that kill the cancer rather than just putting it to sleep. The number one option is chemotherapy but there are others. As you know, I am on a clinical trial investigating the use of Lutetium (a radioligand therapy or RLT) pre-chemotherapy. RLT is a precise targeting of cancer cells that emit PSMA with radiation given intravenously. The problem with Lutetium (a beta emitter) is that while it is good with tumors greater than .5cm it is not very effective at micrometastatic tumours which are energy sheltered and receive low absorbed radiation with Lutetium due to its short path length of approximately of 0.77 mms.
A better option might be Actinium (an alpha emitter) that has proven better outcomes than Lutetium. The BC Cancer Agency has a clinical trial involving Actinium that might still be open to participants. There is also a number of immunotherapy drugs being investigated by the Agency. Have a look on-line and see what is available. If you see something that might benefit you then talk to your oncologist. If you have questions, give me a call. Good luck!
You said "... when... drugs like Xtandi (enzalutamide) and Zytiga (abiraterone) start to fail you need to move to drugs that kill the cancer rather than just putting it to sleep. The number one option is chemotherapy..."
But chemo Taxotere (docetaxel) should be used before, not after, hormone therapy fails. "You can't do chemo after Zytiga helps. You have to start them at around the same time (called "triplet therapy"). The reason is that cancer cells that are not killed by Zytiga go into an impervious state called senescence. Chemo only kills rapidly duplicating cells." -Tall Allen in Healthunlocked: healthunlocked.com/advanced...
I recently started Orgovyx and Zytiga doublet ADT last winter, and chose not to add chemo because I was 81 and did not want to add more side effects. As it has turned out, the side effects of my doublet are insignificant, and I might have been able to tolerate chemo. But that early window has passed, and I am not about to drop the ADT for awhile to try chemo.
One of the reasons why historically chemo has appeared to only provided small benefit is that it has been used at late stage advanced cancer where there are no good options, not just chemo. So called Triplet Therapy is showing that in the right circumstances chemo applied earlier can provide larger benefit.
Your cancer has not been aggressive so far and I think you still have a lot of options. I would definitely ask for a genomics workup which may provide information on selecting treatments matched to your cancer mutations.
Traditionally cancer was treated on a step by step basis. Enforced by insurance companies.
Somebody published some mathematical research.
They found when you are fighting any self replicating biological organism, hitting it hard and early with everything you have slows it down more than staging and escalating your attacks as it grows.
These equations apply as much to a covid epidemic as to prostate cancer.
That mathematical theory has been proven out with countless clinical trials to apply to prostate cancer.
Best practice is to hit it hard early.
It's staged to some extent because of the peculiarities and nuances of the specific treatments.
my hubby started with taxotere first after surgery/radiation (PSA never went down, PET scan showed Mets to spine). He did ok with chemo and it held PSA down from 2018-2020. Next did zytega which held until late 2021. Next Xtandi which did not work. More chemo in 2022. In January 2023, PSA was .8. By October it was the highest to that point, 27. PSMA showed spread of bone Mets to spine, femur and pelvic bones. He started pluvicto in November 2023. After 4 rounds, ALP & PSA both were over 230. A scan showed massive spread from skull to femurs. He is now on Cabazitaxel chemo, indefinitely. The hope is to stop the spread. Right now his PSA has dropped to 59. He is 71 now: had surgery at age 64
they ordered a years worth of treatments since he had such massive spread. If he responds well they may go to every 6 weeks instead of 3. His PSA has gone from 235 to 59 so far so he is responding to it. Feels pretty good but tired easily. We are in our 8th year of treatments and he’s 71 now. He’s a fighter for sure
The trial I was referring to at the B.C. Cancer Agency is NCT06217822 225 Actinium-PSMA-Trillium. I believe it is still recruiting. It is being sponsored by Bayer. Good luck!
Q. When it is considered that Abiraterone plus prednisolone failed? How to make a decision about that?
A. Determining when Abiraterone plus Prednisolone has failed is a critical decision point in managing metastatic prostate cancer. The decision typically involves assessing multiple factors to ensure that the treatment is no longer providing benefit before moving on to alternative therapies. Here’s how this decision is usually made:
### 1. **Rising PSA Levels**
- **PSA Progression:** A key indicator of treatment failure is a consistent rise in PSA levels, despite being on Abiraterone plus Prednisolone. The Prostate Cancer Working Group 3 (PCWG3) criteria define PSA progression as:
- A rise in PSA of 25% or more and an absolute increase of at least 2 ng/mL above the nadir (lowest level reached) on at least two consecutive measurements taken at least one week apart.
- **PSA Doubling Time:** Rapid PSA doubling time (the time it takes for PSA to double) can also suggest that the cancer is progressing despite treatment.
### 2. **Radiographic Progression**
- **Imaging Results:** Progression can also be determined by radiographic evidence, such as the appearance of new lesions or growth of existing lesions on imaging studies (e.g., bone scans, CT scans, or PSMA PET scans). If new metastatic sites appear or existing ones grow, this indicates that the cancer is progressing.
- **Bone Scan or PSMA PET Scan:** The appearance of new bone metastases or visceral metastases on these scans, even if PSA is stable or rising slowly, can indicate treatment failure.
### 3. **Clinical Symptoms**
- **Worsening Symptoms:** The emergence or worsening of symptoms, such as increased bone pain, fatigue, or other signs that the cancer is progressing, can indicate that Abiraterone is no longer effective.
- **Performance Status:** A decline in your overall physical condition or quality of life, particularly if it's related to cancer progression, may also suggest that it's time to switch therapies.
### 4. **Treatment Duration and Expectations**
- **Expected Duration of Response:** On average, patients respond to Abiraterone for about 12-24 months, though this can vary. If the treatment has been effective for a while but starts to lose its impact, it may be time to consider alternative options.
- **Clinical Judgment:** Oncologists will also use their clinical judgment, considering factors like how long you’ve been on the treatment, how rapidly the disease is progressing, and your overall health.
### 5. **Decision Process**
- **Regular Monitoring:** During Abiraterone therapy, you will typically have regular PSA tests, imaging scans, and assessments of symptoms to monitor the effectiveness of the treatment.
- **Consultation with Oncologist:** Your oncologist will evaluate all the data—PSA trends, imaging results, and symptoms—to determine whether Abiraterone is still effective or if it’s time to switch to another treatment.
- **Consideration of Next Steps:** If Abiraterone is deemed to have failed, your oncologist will discuss alternative treatment options, which may include switching to another androgen receptor pathway inhibitor (like Enzalutamide), starting chemotherapy again, considering radionuclide therapy (like Lutetium-177 PSMA), or enrolling in a clinical trial.
### Summary:
Abiraterone plus Prednisolone is considered to have failed when there is clear evidence of disease progression, as indicated by rising PSA levels, worsening symptoms, and/or radiographic progression. This decision is made based on a combination of these factors, guided by regular monitoring and close consultation with your oncologist. If progression is confirmed, the next step is to explore other treatment options that may be more effective in managing your disease at that stage.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.