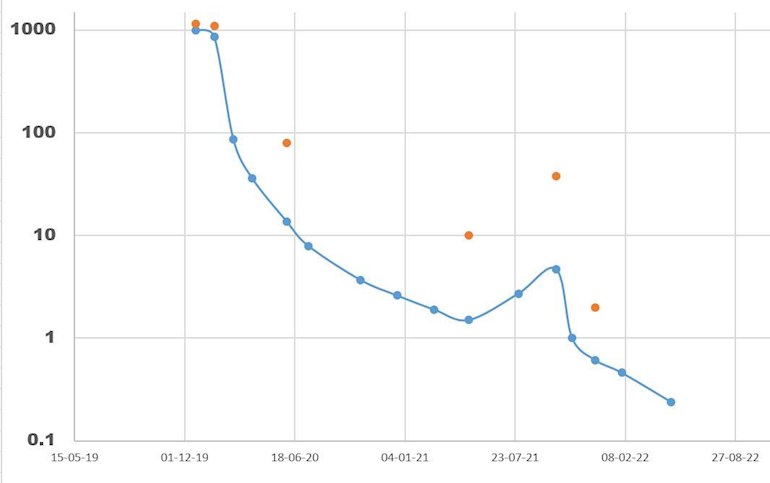
The latest PSA measurement from me shows a nearly 50% decline - which is great news. The decline is marginally greater than the previous period - which is interesting. The only things I have changed is dropping from 160mg/day to 120mg/day Xtandi, and reducing the volume of my food intake (same diet) so as to maintain a stable weight of 68kg. Cant really make any conclusions from this - except that the Xtandi dosage reduction did not reduce the desired effect of the drug for me. Interesting thought - are we generally overmedicinert by the pharma companies???
Heres the latest graph - note the log scale, and that the latest point is a prognosis for next reading in august:
Written by
Stoneartist
To view profiles and participate in discussions please or .
I agree that one has to track it, of course. I'm responding to your comment that just because your PSA is lower, "we are overmedicating." You are making the mistake of confusing PSA with your disease. In all the randomized clinical trials so far, those medications delayed progression and extended survival. Many in the control groups also achieved undetectable PSA, but it didn't last as long, and neither did they.
Fair enough, TA. But how does this man check to see how is cancer is actually doing? Through particular scans? Docs seem to rely very much on PSA, often going years without ordering scans, until it's too late.
Allen - if you remember I did some calculations from the phase 1 clinical studies which showed that Xtandi built up in the blood until it reached saturation level. After that my logic told me that i didnt need such a big dose to maintain saturation level. We know that higher doses have more serious side effects so we are really after the lowest dose which will maintain saturation level - which was why I went from 160mg/day to 120mg/day. The psa curve shows that my latest progression last year was also highly PSA sensitive - which means that for this tumour (s) PSA is a convenient way to track the progression. That the rate of PSA decline was not affected by the dosage reduction I interpret that my reasoning is correct. Of course I know that the current state will be broken sooner or later - and I may or may not be one of the 20% on Xtandi who make it past 2 years before the next progression.
My comment that we are over-medicating relates to the fact that Pharma seem to have a higher focus on the maximum tolerable dose, and a lower focus on the minimum effective dose, and from what I have heard this may be a general problem in the industry.
PSA doesn't show what you think it shows. Many men taking ADT-only in the control groups of those studies reached undetectable PSAs. If you were only trying to reduce PSA that would be fine. But the control group progressed faster and died sooner in spite of their undetectable PSA early on. All you are doing is treating PSA instead of your cancer.
Reason is NOT the way we learn about medical science. ONLY empirical evidence is useful. That's why we depend on the data from randomized clinical trials.
You also don't understand dosing. For most medicines, there is a dose response: higher doses have more effectiveness. Dose is found by looking at the S-curve - to maximize effectiveness, we want the dose to be at the end of the steep part of the S-curve. Sometimes, the dose is intolerable at that point and we have to settle for lesser effectiveness in order to have side effects we can live with. So the maximum tolerable dose is the only important determinant. The minimum effective dose gives a much lower effect. You have to understand the S-curve.
You are also wrong about lowering the dose after steady state saturation is reached. At that point, one does NOT get more side effects - the excess drug is eliminated and does not cause extra side effects.
I should add that you have to consider active metabolites of enzalutamide too. Sometimes the metabolites have a more important effect than the initial medicine.
yes but until you do the trials you wont know if the metabolites have a good or a bad effect. The phase 1 dosage trails found that dosages of Xtandi (it was called something else then) gave increasingly negative side effects for dosages 180mg/day and over. Thats why they settled on 160mg/day as a standard dose. They established the half-life and the saturation concentration in those tests.
I follow the SOC and start with 160mg/day. My logic and reasoning (yes - these play an important place in all science and they direct which tests (trails) are worth pursuing) tells me that I reach saturation on 160mg, and can maintain saturation on 120mg. My oncologist agrees so I made a trial between two PSA readings (3 month intervals) - the first interval on 160mg gave a sharp decrease in tumour activity - as measured by PSA. the next 3 month period I was on 120mg - and the decrease in tumour activity continued at the same rate. This indicates that the 120mg dose was just as effective as the 160mg dose since it is unlikely that the PSA decrease is caused by anything else that the Xtandi treatment. This is simple science - a test performed on one man - me. I say indicates - not proves - if you want proof you need to do a phase 3 clinical trial - but the indication is so strong - and backed by reasoning- so thats what I have chosen - and will continue with 120mg dose until Xtandi fails as it surely will
I fail to see why you object to this simple argument - it sounds like you mean I should stay on 160mg - even when my oncologist supports me.
If I could obtain a steady, but measurable PSA nadir I could test for other factors If necessary, though I guess that at these low levels changes in PSA could be caused by many things. This case I am using a consistent fall over two periods - it will be interesting to see what the next reading is in august.
You are measuring the activity of your cancer by PSA - this is a mistake. I've told you this several times and you can't seem to comprehend it. They do not approve drugs based on PSA effect. It is only used as a screener - if it has no effect it is rejected. You are playing games with your life.
If the pharmaceutical mfr (who I suggest you contact) thought 120 mg was an adequate maintenance dose, they would have made it in that dose. They would charge the same (the price of most expensive pharmaceuticals have nothing to do with the cost of chemicals - but that is a different discussion) and make the same amount of money.
So true - but my Oncologist backed me up on this dose reduction which I suggested. I was having leg cramps and now they have completely gone. We have had previous discussions about this on this site
Did you reduce dose at the advice of your Oncologist? As it seems to me things like this boil down to, do you trust your doctor as being highly competent, keeping up with the latest data, or not? If not, switch doctors as offering the most informed expert advice is what they are paid to do.
Some of us don't have much of a choice. 160 mg made me a complete invalid.... 120 mg and I could function with restrictions. 80 mg and my life came back, but my neuropathy continues and will probably never get better. 3 1/2 years of xtandi before BCR.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.