I was diagnosed with Graves and hyperthyroidism in Jan 22, having my levels go up and down like a yo-yo the endocrinologist suggested having a thyroidectomy. Which I had in Sept 23, after the op I was prescribed 150mcg of levothyroxine, and after 6 weeks a post op blood test, I hadn’t realised that no one looked at the results and I overprescribed and hyper again with levels of over T4 at 32 Pmol/L - I was told to drop the dosage to 100mcg immediately by the GP but then the endocrinologist said to reduce to 125mcg not 100mcg but after 6 weeks T4 was still high at 26.5 Pmol/L so the GP reduced again back to 100mcg so my last test in March showed T4 normal level at 19.8 Pmol/L however I still have zero reading on TSH. So I agreed with the GP to stay on 100 mcg as I was feeling a bit more human after two years of feeling dreadful.
Now my Endocrinologist wants to reduce to 100mcg and 75mcg on alternate days so average of 82.5 - but I’m worried that I will go hypo.
Really fed up of yo-yo ing between hypo and hyper and feeling completely exhausted and drained with it all.
I have a blood test next week and have asked my GP to wait till this result is in before any action is taken.
The GP and Endo want to reduce the dose to try and kick start my TSH production, but I need to be able to work and hold down a full time role and they just don’t seem to understand that feeling completely exhausted all the time is really affecting my mental well-being as well. Living a life for over two years where I work and sleep and not much else is.
When does the TSH go back to “normal” range after a thyroidectomy, and should the Endocrinologist keep reducing my levothyroxine even though showed I was in normal range in March especially without checking where my levels are now.
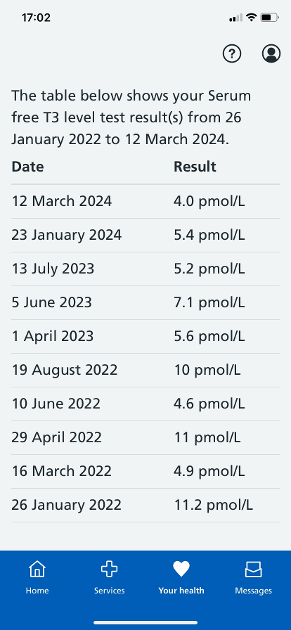
Result of T3 &T4 above, TSH is 0
Any advice would be appreciated, has anyone had a similar experience ?
Written by
Gabanna
To view profiles and participate in discussions please or .
Ask them why they want to 'kick-start' your pituitary into making TSH again, when you haven't got a thyroid to stimulate?!?
If they reply with something about hearts and bones, they're just showing their ignorance. TSH has nothing to do with hearts or bones. You don't need it.
How long were you hyper with a suppressed TSH? Because if it was over a period of some time, it might never rise again, because the HPT axis has become down-regulated by the Graves'. And they should know that.
But, I assure you, it's nothing to worry about, except for ignorant doctors who keep reducing your dose. They should not do that. They are going to make you ill. The most important number is the FT3, and I see that yours is now too low as it is. Reducing your levo any further will make you hypo. So, just refuse.
Hi - I was diagnosed in Jan 22 and was hyper until recently even after the thyroidectomy due to overprescribed levothyroxine at 150mcg for 3 months. I’ve been TSH suppressed since diagnosis.
And yes they are mentioning heart and bones !! That’s the endocrinologist rather than GP, and I thought that’s was mainly due to Graves’ disease and thyrotoxicosis.
I would imagine your TSH was suppressed long before your diagnosis if you had Graves'.
You're right about the risk to hearts and bones being due to thyrotoxicosis, but what causes the risk is the high FT3, not the low TSH. But they cannot see the difference between a suppressed TSH due to the high FT3 in Graves', and a suppressed TSH due to taking exogenous hormone.
If I were you, I'd just refuse to reduce any further just for the sake of something you don't even need!
I did try to put all my test results and ranges in here, but it only added one photo. T 3 range is 3.1 to 6.8 and my result was 4 in March. T4 range is 11 to 22 and my result was 19.8. I’m
Currently taking 100mcg and I don’t always get the same brand from the chemist.
I will ask for my vit levels, calcium, folate and ferritin are tested. I can ferritin was tested before and was the low end of normal but can’t see any others. I’ll also ask if they can test my TraB levels as well but I think the endo has to request these.
I’m suffering from extreme fatigue which is making my day to day life really difficult as I have no option but to work full time. I cannot currently afford to have any private tests done either.
It can take a long time for TSH to recover, if it does ncbi.nlm.nih.gov/pmc/articl.... One of the reasons is that Graves' antibodies feedback to the pituitary suppressing TSH. So, TSH is unlikely to recover until at least your TRAB antibodies have fallen to low levels.
Graves is an Auto Immune disease for which there is no cure, and simply removing the thyroid - the target of the immune system attack - a somewhat simplistic solution -
The thyroid is a major gland responsible for full synchronisation of the body - from physical stamina, through to emotional, mental, psychological and spiritual well being - your inner central heating heating system and your metabolism.
So now you still have Graves Disease but are primary hypothyroid and must be dosed and monitored on your Free T3 and Free T4 blood test results and not a TSH.
Graves can wax and wane throughout your life, and the Graves antibodies maybe circulating in your blood for the rest of your life - and they tend to ' sit on ' and get ' stuck on ' the TSH receptors - driving down the TSH marker - which in turn triggers the production of thyroid hormones and why you became hyperthyroid in the first instance.
But since you have had a medical intervention and definitive treatment - there now is no automatic, natural thyroid production - the Hypothalamic - Pituitary - Thyroid feedback loop broken - the HPT axis down regulated and your TSH a totally unreliable measure of anything
We generally feel best when our T4 is in the top quadrant of its range with the T3 tracking just behind at around 60/70 % through its range.
T4 - Levothyroxine is a pro-hormone and needs to be converted in the body into T3 which is the active hormone that runs the body - much like petrol runs a car - and you likely need a full tank to get you through a full day.
Conversion of T4 into T3 can be compromised by non optimal levels of core strength vitamins and minerals so suggest you get ferritin, folate, B12 and vitamin D as if these are not maintained at optimal levels - which we can advise on - your health likely unnecessarily compromised further..
A fully functioning working thyroid would be supporting you on a daily basis with trace elements of T1. T2 and calcitonin + a measure of T3 at around 10 mcg + a measure of T4 at around 100 mcg - with T3 said to be around 4 times more powerful than T4.
Some people can get buy on T4 - Levothroxine only.
Others find T4 seems to stop working as well as it once did and that by adding in a little T3 - likely at a similar dose to that their thyroid once supported them with - they are able to restore T3/T4 hormonal balance and health and well being restored.
Some can't tolerate T4 at all and need to take T3 - Liothyronine only -you can live without T4 but you can't function or live without T3.
Whilst others find their health restored better taking Natural Desiccated Thyroid which contains all the same known hormones as that of the thyroid gland and derived from pig thyroids, dried and ground down into tablets referred to as grains.
Up until around 2000 all the above treatment options were available from your primary care doctor if T4 - the cheapest option - didn't restore health and well being -
currently you need a referral to endocrinology to be assessed for any other treatment option and it does appear to be something of a postcode lottery with ICB / CCG financial constraints rather than medical need being followed.
Obviously if you can afford to go privately you are looking at a very different landscape.
The most rounded of all I researched for Graves Disease is that of Elaine Moore - books and website - elaine-moore.com
Barbara S Lougheed - Tired Thyroid - from Hyper - to Hypo - to Healing - Breaking the TSH rule:
How are your eyes - are they dry, gritty, light sensitive ?
I'm with Graves post RAI thyroid ablation 2005 - if interested you can read my Profile page and everything I've written on this open forum - just press the icon alongside my name - and to find your home page just press the Profile icon on this page which is sitting top right for me on my laptop alongside My hub - Chat - Post and Alert icons.
I now see we have a T3 at 4 ( 3.10 - 6.80 ) and a T4 at 19.80 ( 11 - 22.00 ) in March just gone :
So your T4 is at a good level and around 80% through its range but your T3 is only around 25% through it's range showing very poor conversion.
and when on T4 monotherapy - both these 2 vital hormones need to be balanced within the range at around a 1/4 ratio T3/T4.
The accepted conversion is said to be 1 / 3.50 - 4.50 T3/T4 - with most people feeling at their best when they come in this little conversion ratio at 4 or under -
So if I divide your T4 reading by your T3 reading I'm getting your conversion coming in at 4.95. so wide of the centre mark and showing poor conversion of T4 into T3.
I've seen worse - some up in the 6's - one in the 8's - mine came in at 5.50
Optimal vitamins and minerals will help improve your conversion - I now aim for a ferritin at around 100 - folate 20 - active B12 125 ( serum B12 500++ ) and vitamin D at around 125.
There is no point asking for your TRab blood tests to be rerun - it's doesn't matter or change anything - you have had definitive treatment and your thyroid removed and your own natural power supply of thyroid hormones ' cut ' and been switched from automatic thyroid hormone production to manual which you take every day in the form of thyroid hormone replacement.
You will more than likely need to ask for a referral to an endocrinology to assess your need for T3 - and be prescribed a combination of T3 and T4 thyroid hormones to restore this vital balance in order to give you back your health well being and your ' you ' :
I don't know where you live in the country - as it has become something of a postcode lottery getting any additional treatment options other than T4 prescribed - have you now been discharged by endocrinology - and back with your primary care provider - or still under the hospital ?
Thyrod UK - the charity who supports this patient to patient forum holds as list of recommended thyroid specialists and endos - both NHS and Private - so just contact admin @ thyroiduk.org - and get the list - and just see if there is anyone there who might be local to you and worth being referred to -
If your current NHS endo team - if you have one - are obsessed with TSH values - that when with Graves may never recover - and if being dosed and monitored on just a TSH reading taking centre stage - this will put you in an ever decreasing circle of wellness.
Centre stage in all blood tests must be your Free T3 - and currently it is much too low to allow you to function, be well and back to your ' normal ' :
If you go into openprescribing.net and then hospital and / or doctor's surgery - you can see by ICB / CCG area what's going on- and also see by doctors surgery if T3 is being prescribed and your primary care provider supportive of prescribing other options to just T4 monotherapy.
Just enter Liothyronine for the T3 drug :
If looking to try Natural Desiccated Thyroid - the other and original treatment successfully used to treat hypothyroidism for over 100 years as mentioned in my post last night - this is even harder to get prescribed on the NHS :
Just enter Armour - as the drug - which is the leading most expensive brand that the NHS is meant to still prescribe on a ' named patient only ' prescription.
P.S.
Maybe start a new post asking for feedback on your catchment area - and see who/what other forum members have already found out and if there is a thyroid friendly specialist within your catchment area -
and there are always video consults - but guess you may first like a face to face with someone to help you ?
Oh poor you. That is appalling treatment. The best thing you can do for yourself is learn how to read labs with the help of others here.
A long term suppressed TSH may not rise. Many of us here medicated for both hyperthyroidism and hyperthyroidism only function well with a low/suppressed TSH. Some members have had their thyroid med dose manipulated to an extent they have become symptomatic but the TSH has remained unaffected.
For a long time medics have shouted about TSH being needed for heart and bone health but a lack of scientific evidence has led patients to overlook this claim and ensure thyroid hormones levels that best look after the heart and bones are adhered to, eg not too high (bone-thyrotoxicosis) and not too low. However, research is now immerging showing some TSH being required for best bone health. ‘a low TSH “may inhibit proliferation and matrix synthesis in the chondrocytes that regulate collagen use in bone and connective tissue’.
This makes patients more vulnerable to not only enforced thyroid meds dose reductions but bone conditions such osteoporosis. However, the correct amount of thyroid hormone is also imperative for correct balance of osteoblasts (bone formation) V osteoclasts (bone breakdown) and so healthy bones. Osteoblasts have been found to express both thyroid hormone conversion enzymes in bone (D2 - activating, and D3 - deactivating). To some extent this allows some protection to the effects of a low TSH.
Therefore, I continue to think at present we should ignore a low TSH until more evidence can be presented.
Hi there, I had my thyroid removed due to Graves 7 years ago. My TSH has always been 0.01 ever since. I have a constant battle with GPs because of this. Every time they try and reduce and I just say, I feel fine and do not feel over medicated and am willing to take the risk, then they leave me alone into the next blood test. I do worry about it, but my T3 and T4 are in range, in fact in the lower end. Hope this helps 😊x
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")