Thanks for everyone’s help with my questions already.
I am in a thyroid group on Facebook and they have told me that if you are on levothyroxine medication for an under active thyroid then you should aim for your tsh to be as close to zero as possible, because the levothyroxine is meant to completely replace the bodies requirement for T4. Is that right? My endo said she’s aiming for me to get close to 1. I’m not sure if I should push for more levo to try to reduce my TSH further.
Latest results:
18th Jan - taken at 9am with 24 hours after last levo dose
TSH 1.94
T4 15.7
T3 4.7
My endo didn’t give me the ranges. In hindsight I should have asked at the appointment but I was expecting to be sent the results formally by email afterwards. It was my first appointment with that private hospital.
29th Jan taken at 11am with 5 hours after last levo dose.
TSH 1.45 (0.35-5.5)
This was an NHS test as part of a range of recurrent miscarriage tests but it didn’t test any other thyroid levels
It seems to make sense that my TSH was lower on the test where I had taken the levothyroxine more recently, but my endo said it doesn’t work like that. Is that right?
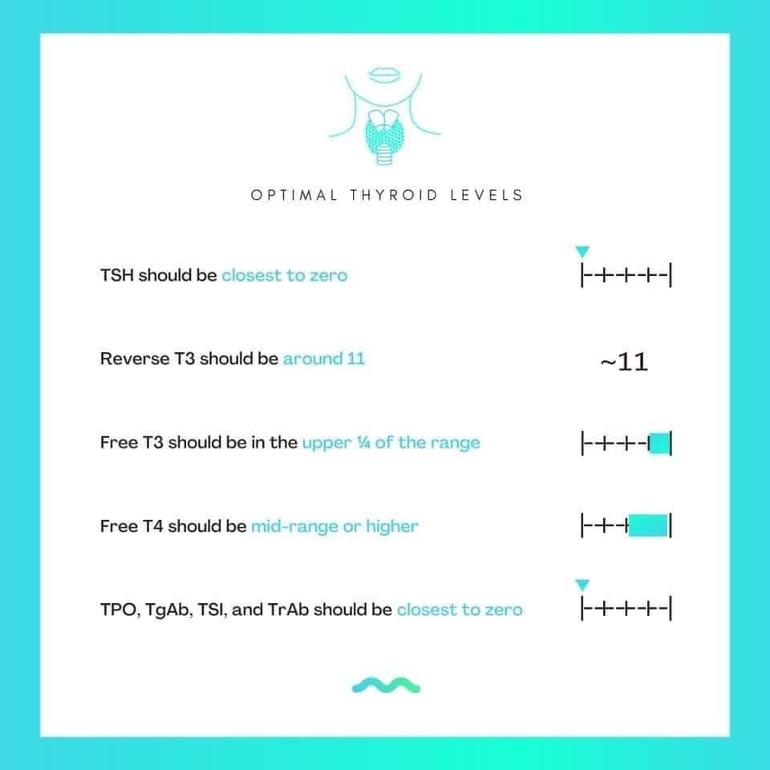
I have attached the levels that the Facebook group say we should be aiming for. Are they right?
Thank you in advance.
Written by
Treesandleaves
To view profiles and participate in discussions please or .
Bloods should be retested 6-8 weeks after each dose change or brand change in levothyroxine
For full Thyroid evaluation you need TSH, FT4 and FT3 tested
Also both TPO and TG thyroid antibodies tested at least once to see if your hypothyroidism is autoimmune
Very important to test vitamin D, folate, ferritin and B12 at least once year minimum
About 90% of primary hypothyroidism is autoimmune thyroid disease, usually diagnosed by high TPO and/or high TG thyroid antibodies
Autoimmune thyroid disease with goitre is Hashimoto’s
Autoimmune thyroid disease without goitre is Ord’s thyroiditis.
Both are autoimmune and generally called Hashimoto’s.
Significant minority of Hashimoto’s patients only have high TG antibodies (thyroglobulin)
Low vitamin levels are extremely common when hypothyroid, especially with autoimmune thyroid disease
20% of autoimmune thyroid patients never have high thyroid antibodies and ultrasound scan of thyroid can get diagnosis
In U.K. medics hardly ever refer to autoimmune thyroid disease as Hashimoto’s (or Ord’s thyroiditis)
Recommended that all thyroid blood tests early morning, ideally just before 9am, only drink water between waking and test and last dose levothyroxine 24 hours before test
This gives highest TSH, lowest FT4 and most consistent results. (Patient to patient tip)
Private tests are available as NHS currently rarely tests Ft3 or all relevant vitamins
Testing options and includes money off codes for private testing
I have very high TPO Antibodies and am currently taking 75 mg of levothyroxing five days a week and 100mg twice a week.
I've had vitamins tested recently:
Vitamin D came out at 55 (50-200) nmol/L so my endo has since increased my vitamin D to 3000 iu per day.
Ferritin was 31.8 (13-150) µg/L
Folate was 42.7 (8.83-60.8) nmol/L
B12 was 453 (145-569) pmol/L
Do you have any knowledge about whether it is correct to aim for TSH being as close to zero as possible? And do you know if those 'Optimal ranges' that are being suggested in the picture are correct?
"if you are on levothyroxine medication for an under active thyroid then you should aim for your tsh to be as close to zero as possible, because the levothyroxine is meant to completely replace the bodies requirement for"
This is completely wrong. When the axis is working correctly a healthy person will, on average, have a TSH around say 1.5 to 2.0. Someone on levothyoxine monotherapy would need a TSH to be say 0.5 to 1.0 to achieve the same fT3. This works for many people. I no longer agree with it because it gives higher fT4 levels that are associated with cancer and cardiac mortality. I think everyone should get a little T3 to help keep fT4 in the lower half of its reference interval.
The above applies to people with straightforward primary hypothyroidism. Some patients have other thyroid hormone problems and need more hormone, especially T3.
TSH not only stimulates the thyroid (and other organs) but is also subject to negative feedback from fT3 and fT4. So, in healthy individuals it is a good measurement of combined fT3, fT4 status in each individual. In healthy people a TSH near zero would signal a problem. The same applies to most thyroid patients, thus it should not be a target.
TSH is a bit like electricity, a good servant but poor master.
That's a weird diagram if it's meant to be someone on levo only. You'd have a hard job to get your FT3 up in the top quartile if the FT4 is only around mid-range. Not sure it's doable.
Be very wary of Facebook thyroid groups. They include some very weird people with some very strange ideas about thyroid, and not much actual knowledge. After having tried several, I now avoid them like the plague!
It seems to make sense that my TSH was lower on the test where I had taken the levothyroxine more recently, but my endo said it doesn’t work like that. Is that right?
Your endo is right. The TSH works much more slowly than the thyroid hormones. It can take days for the TSH to react to a change in dose, it doesn't react to the time of day you take your levo.
It does, however, fluctuate throughout the day, being highest at midnight and then dropping to its lowest around midday. Which is why we always recommend having the blood draw before 9 am.
Taking your levo too close to the blood draw will just affect the FT4 level.
The idea that everyone on thyroid hormone replacement should be "aiming" to get their TSH close to 0 is not really correct , no .
It's far too simplistic a statement, showing lack of understanding of the complexities and individualities involved .
I have linked to 3 posts below, which contain links to the detail required for much better understanding of the subject and i would politely suggest the fb group author should do some more homework and read them all thoroughly before promoting TSH 0.00 as an ideal target for everyone.
Firstly , there is absolutely nothing wrong with having TSH around 1ish IF the patient feels and functions well there, and if their fT4 / fT3 levels look reasonable...... these patients should not be advised to increase their dose purely for the aim of bringing their TSH closer to 0.
For some, the dose which allows them to function ok may leave their TSH a little below reference range but not totally supressed' (ie. it's somewhere between 0.04 and 0.4 approx) .... these people should not be told to aim for closer to 0.
Some people would experience symptoms of overmedicated on a dose that gave them high-end fT4 and very low /supressed TSH ...... these people should obviously not be told to aim for TSH close to 0. (eg. i find i am generally fine at 0.04 / 0.05 ish but felt godawful at 0.01)
Yes , it's definitely true that some DO find they need a level of T4/ T3 that has the consequence of totally supressing TSH, but supressing the TSH is not our aim .... having levels of T4/T3 that enable us to function well is the aim .. a totally supressed TSH is an (unfortunate) bi-product of this in some people.
Some people will function best with levels of fT4/fT3 that do not supress their TSH as low as 0, and IF this balance can be achieved , then it is probably preferable.
In an ideal world we want to be keeping our TSH at least 'measurable' (eg. over 0.04 for the sake of argument)
because:
1) the TSH level plays a small role in helping with conversion of T4 to T3 , therefore having 'some' TSH is no bad thing........ and
2) because having high end fT4 with a TSH BELOW 0.04 has been associated with some increased risks.
so 'aiming' for fT4 at 99% and TSH at 0.00 is really not good advice ....sure , some people find (after giving lower doses a fair trial and finding they couldn't function) that they need a dose that gives these levels ~ and those in that position must make a judgement call ~ balancing their need for quality of life/ function 'now', with their willingness to accept the potential for some increased risks that may /may not happen in their future.
Everyone is unique - it’s all about how I am feeling that determines where I want to be on a range. For me, my previous doctor was keeping me too low on TSH range and I kept sliding to a hyper state, which I detest and all the scary symptoms that went with that. My Levo kept needing to be reduced year after year because this was happening.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")