Hi Looking for some guidance please. I was picked up on a blood test about 18 months ago and am now taking Levothyroxine. I haven't seen much improvement (or side effects) but am now considered "managed" by the GP as my TSH is now within range. I had asked for further test and these were declined so I got some done privately (below).
I made another GP appointment to seek their opinion, and after being berated for getting private blood tests, was told that even though my antibodies were well out of range the condition was managed. The test also showed high cortisol, which I was told was due to the stress of a blood test (rite!) and also vit. D is borderline.
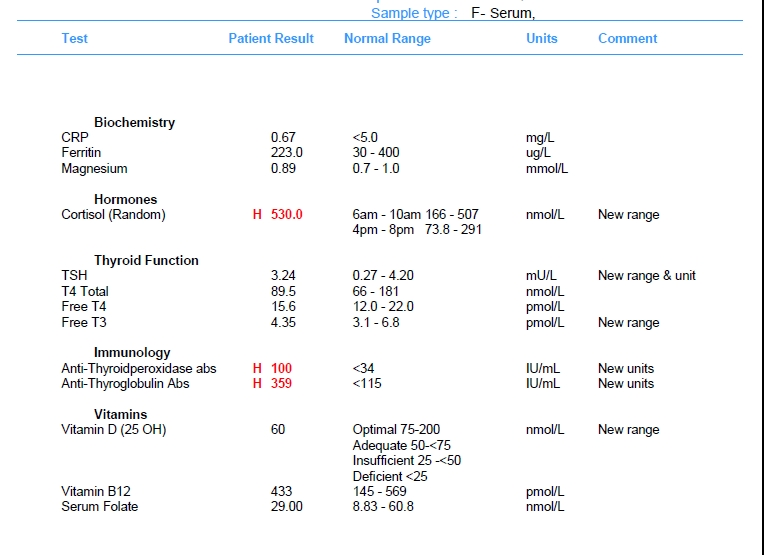
Blue Horizon Doctor's feedback "The serum cortisol is high. Cortisol rises in response to stress, but it will also rise in those taking steroids (even as creams or asthma inhalers). Persistently raised cortisol levels may indicate underlying Cushing's disease, but further testing would be required to diagnose (or rule out) this condition. Repeat testing would be advisable to determine whether it is a sustained rise, and you may wish to consider 24 hour testing of saliva cortisol levels (via a home testing kit).The thyroid function is currently normal. The positive thyroid antibody result, however, increases the possibility of your having or ultimately developing autoimmune thyroid disease, such as Hashimoto's thyroiditis or Grave's disease."
So I am going back to the senior GP for round 2 and wondered if anyone had any input. Should my dose be higher? Should I be on something else? Is the cortisol significant?
Many thanks
Written by
StanleyThyroid
To view profiles and participate in discussions please or .
- I am on 50ug Almus Levothyroxine -its always been that one. Test was done 9am without taking anything that morning.
- At the moment I take 2 x Centrum Advance 50+ Multivitamin & Mineral Tablets, L-glutamine, Magnesium Citrate at night and also a nutropic called MindLab Pro. I also use testosterone gel. I had been taking B12 supplements until this test came back and said my levels were fine, which seems I may still need.
I will definitely as k for the dose to be upped. Is it reasonable that the GP would approve a test very 6 weeks - where I am they only seem to want to do TSH.
In the majority of patients 50-100 μg thyroxine can be used as the starting dose. Alterations in dose are achieved by using 25-50 μg increments and adequacy of the new dose can be confirmed by repeat measurement of TSH after 2-3 months.
The majority of patients will be clinically euthyroid with a ‘normal’ TSH and having thyroxine replacement in the range 75-150 μg/day (1.6ug/Kg on average).
The recommended approach is to titrate thyroxine therapy against the TSH concentration whilst assessing clinical well-being. The target is a serum TSH within the reference range.
……The primary target of thyroxine replacement therapy is to make the patient feel well and to achieve a serum TSH that is within the reference range. The corresponding FT4 will be within or slightly above its reference range.
The minimum period to achieve stable concentrations after a change in dose of thyroxine is two months and thyroid function tests should not normally be requested before this period has elapsed.
Thank you for this, still reading through everything! On your calculation ( and with weight now having crept up to 95kg) implies that I should be on 150ug (currently 50). Looks like a big jump - must that be done in 25s?
Your antibodies are high this is Hashimoto's, (also known by medics here in UK more commonly as autoimmune thyroid disease).
Hashimoto's affects the gut and leads to low stomach acid and then low vitamin levels
Low vitamin levels affect Thyroid hormone working
Poor gut function can lead leaky gut (literally holes in gut wall) this can cause food intolerances. Most common by far is gluten. Dairy is second most common.
A trial of strictly gluten free diet is always worth doing
Only 5% of Hashimoto’s patients test positive for coeliac but a further 81% of Hashimoto’s patients who try gluten free diet find noticeable or significant improvement or find it’s essential
Similarly few months later consider trying dairy free too. Approx 50-60% find dairy free beneficial
Hashimoto’s and leaky gut often occur together
Both dairy and gluten are inflammatory foods
A strictly gluten free diet helps or is essential due to gluten intolerance (no test available) or due to leaky gut and gluten causing molecular mimicry (see Amy Myers link)
Changing to a strictly gluten free diet may help reduce symptoms, help gut heal and may slowly lower TPO antibodies
While still eating high gluten diet ask GP for coeliac blood test first (as per NICE guidelines)
or buy test online for under £20, just to rule it out first
Assuming test is negative you can immediately go on strictly gluten free diet
(If test is positive you will need to remain on high gluten diet until endoscopy, maximum 6 weeks wait officially)
Trying gluten free diet for 3-6 months. If no noticeable improvement then reintroduce gluten and see if symptoms get worse
The predominance of Hashimoto thyroiditis represents an interesting finding, since it has been indirectly confirmed by an Italian study, showing that autoimmune thyroid disease is a risk factor for the evolution towards NCGS in a group of patients with minimal duodenal inflammation. On these bases, an autoimmune stigma in NCGS is strongly supported
In summary, whereas it is not yet clear whether a gluten free diet can prevent autoimmune diseases, it is worth mentioning that HT patients with or without CD benefit from a diet low in gluten as far as the progression and the potential disease complications are concerned
Despite the fact that 5-10% of patients have Celiac disease, in my experience and in the experience of many other physicians, at least 80% + of patients with Hashimoto's who go gluten-free notice a reduction in their symptoms almost immediately.
I have been gluten free for about 25 years now. I was diagnosed at a time before anyone had really heard about it and coming off gluten definitely made a big difference to my health. I am also intolerant to other grains and processed food, so I have quite a restricted diet.
I appreciate all the links and I will take my time to look at them.
This forum has proved invaluable already. Thanks again
Looking at thyroid results your are simply undermedicated. Although your results fall within the normal range you need them to be more OPTIMAL.
Free T4 (fT4) 15.6 pmol/L (12 - 22) 36.0%
Free T3 (fT3) 4.35 pmol/L (3.1 - 6.8) 33.8%
Your FT4 should be much higher as should your FT3 for you to feel better. You seem to be converting well. Insist on a 25mcg dose increase when you see your GP, your TSH should be closer to when and even slightly under 1.
To get vitamins raised buy some D3 & K2. There is a calculator here to work out how much you need to take. grassrootshealth.net/projec...
Your folate isn't terrible but could use a boost. It's recommended to take a B complex to keep all B's in balance, such as Thorne Basic B. Shop around for best price.
First question has to be - do you do your tests as we advise:
* Book the first appointment of the morning, or with private tests at home no later than 9am. This is because TSH is highest early morning and lowers throughout the day.
In fact, 9am is the perfect time, see first graph here, it shows TSH is highest around midnight - 4am (when we can't get a blood draw), then lowers, next high is at 9am then lowers before it starts it's climb again about 9pm:
If we are looking for a diagnosis of hypothyroidism, or looking for an increase in dose or to avoid a reduction then we need TSH to be as high as possible.
* Nothing to eat or drink except water before the test - have your evening meal/supper as normal the night before but delay breakfast on the day of the test and drink water only until after the blood draw. Certain foods may lower TSH, caffeine containing drinks affect TSH.
* If taking thyroid hormone replacement, last dose of Levo should be 24 hours before blood draw. If taking NDT or T3 then last dose should be 8-12 hours before blood draw, split dose and adjust timing the day before if necessary. This avoids measuring hormone levels at their peak after ingestion of hormone replacement. Take your thyroid meds after the blood draw. Taking your dose too close to the blood draw will give false high results, leaving any longer gap will give false low results.
* If you take Biotin or a B Complex containing Biotin (B7), leave this off for 7 days before any blood test. This is because if Biotin is used in the testing procedure it can give false results (most labs use biotin).
These are patient to patient tips which we don't discuss with phlebotomists or doctors.
Also, take your Levo on an empty stomach, one hour before or two hours after food, with a glass of water only, no tea, coffee, milk, etc, and water only for an hour either side, as absorption will be affected. Take any other medication and supplements 2 hours away from Levo, some need 4 hours.
Should my dose be higher?
If you did the test as above to give a measure of your normal circulating hormone then in my opinion, and most likely the opinion of everyone else here, yes your dose should be higher.
The aim of a treated hypo patient on Levo only, generally, is for TSH to be 1 or below with FT4 and FT3 in the upper part of their reference ranges, if that is where you feel well.
Your TSH is too high, your FT4 is 36% through it's range and your FT3 is 33.78% through range, so you can see that your actual thyroid hormones (FT4 and FT3) are low in range. All this is telling us that you are undermedicated.
Your raised thyroid antibodies confirm autoimmune thyroid disease (Hashimoto's) which is the most common cause of hypothyroidism and is where the immune system attacks the thyroid and gradually destroys it.
Fluctuations in symptoms and test results are common with Hashi's.
Most doctors dismiss antibodies as being of no importance and know little or nothing about Hashi's and how it affects the patient, test results and symptoms. It would be best to read, learn, understand and help yourself where Hashi's is concerned.
Some members have found that adopting a strict gluten free diet can help, although there is no guarantee.
Gluten contains gliadin (a protein) which is thought to trigger autoimmune attacks so eliminating gluten can help reduce these attacks.
You don't need to be gluten sensitive or have Coeliac disease for a gluten free diet to help.
Supplementing with selenium l-selenomethionine 200mcg daily is said to help reduce the antibodies, as can keeping TSH suppressed.
Hashi's and gut absorption problems tend to go hand in hand and can very often result in low nutrient levels or deficiencies so it's important to check these and supplement where necessary.
Continued in a new post due to word count restrictions.
am now considered "managed" by the GP as my TSH is now within range.
The aim is not to get the patient "within range", it's to alleviate symptoms and give the dose of Levo that achieves that, bearing in mind that FT4 and FT3 should be kept in range. Unfortunately NICE guidelines don't give "target" levels but this is what is said
Tests for follow-up and monitoring of primary hypothyroidism
1.4.1 Aim to maintain TSH levels within the reference range when treating primary hypothyroidism with levothyroxine. If symptoms persist, consider adjusting the dose of levothyroxine further to achieve optimal wellbeing, but avoid using doses that cause TSH suppression or thyrotoxicosis.
As for your cortisol, it is slightly over range and I do agree that it would be worth doing a 24 hour salive test; however, I don't recommend doing it with Blue Horizon. This is because it only tests cortisol and for a full picture to determine the stage of adrenal fatigue (if present) then you need cortisol plus DHEA. You can get a cortisol plus DHEA test with Regenerus and it costs less than the Blue Horizon test:
click on the second link for the adrenal function test which takes you to Regnerus' website and you will see the test ADRENAL FUNCTION (5)
You name ThyroidUK as your "practioner". Results are sent direct to you.
CRP is an inflammation marker, your level is nice and low and shows no inflammation.
Ferritin can be raised when inflammation is present, as your CRP shows no inflammation then your ferritin is likely to be a true result and is good.
Magnesium - Testing magnesium is unreliable. About 99% of magnesium is stored in bone, muscles and soft tissues, leaving about 1% in the blood. So testing what's in the blood isn't giving an accurate picture of our magnesium status.
A red cell magnesium test is the better indicator of magnesium status, not the standard serum magnesium test. The red cell test is expensive and requires phlebotomy which is why it's not included in these bundles.
Vit D: 60nmol/L
You might want to check out a recent post that I wrote about Vit D and supplementing:
The Vit D Council, the Vit D Society and Grassroots Health all recommend a level of 100-150nmol/L (40-60ng/ml), with a recent blog post on Grassroots Health mentioning a study which recommends over 125nmol/L (50ng/ml).
So now you look at how much is needed to reach 50ng/ml and you'll see that they suggest 3,700iu per day, nearest to buy is 4,000iu.
Once you've reached the recommended level then a maintenance dose will be needed to keep it there, which may be 2000iu daily, maybe more or less, maybe less in summer than winter, it's trial and error so it's recommended to retest once or twice a year to keep within the recommended range. This can be done with a private fingerprick blood spot test with an NHS lab which offers this test to the general public:
Doctors don't know, because they're not taught much about nutrients, but there are important cofactors needed when taking D3. You will have to buy these yourself.
D3 aids absorption of calcium from food and Vit K2-MK7 directs the calcium to bones and teeth where it is needed and away from arteries and soft tissues where it can be deposited and cause problems such as hardening of the arteries, kidney stones, etc. 90-100mcg K2-MK7 is enough for up to 10,000iu D3.
D3 and K2 are fat soluble so should be taken with the fattiest meal of the day, D3 four hours away from thyroid meds if taking D3 as tablets/capsules/softgels, no necessity if using an oral spray.
For D3 I like Doctor's Best D3 softgels, they are an oil based very small softgel which contains just two ingredients - D3 and extra virgin olive oil, a good quality, nice clean supplement which is budget friendly. Some people like BetterYou oral spray but this contains a lot of excipients and works out more expensive.
For Vit K2-MK7 my suggestions are Vitabay, Vegavero or Vitamaze brands which all contain the correct form of K2-MK7 - the "All Trans" form rather than the "Cis" form. The All Trans form is the bioactive form, a bit like methylfolate is the bioactive form of folic acid.
Vitabay and Vegavero are either tablets or capsules.
Vitabay does do an oil based liquid.
Vitamaze is an oil based liquid.
With the oil based liquids the are xx amount of K2-MK7 per drop so you just take the appropriate amount of drops.
They are all imported German brands, you can find them on Amazon although they do go out of stock from time to time. I get what I can when I need to restock. If the tablet or capsule form is only in 200mcg dose at the time I take those on alternate days.
If looking for a combined D3/K2 supplement, this one has 3,000iu D3 and 50mcg K2-MK7. The K2-MK7 is the All-Trans form
Magnesium should be taken 4 hours away from thyroid meds and as it tends to be calming it's best taken in the evening. Vit D should also be taken 4 hours away from thyroid meds. Vit K2-MK7 should be taken 2 hours away from thyroid meds. Don't take D3 and K2 at the same time unless both are oil based supplements, they both are fat soluble vitamins which require their own fat to be absorbed otherwise they will compete for the fat.
Not bad but could be better. According to an extract from the book, "Could it be B12?" by Sally M. Pacholok:
"We believe that the 'normal' serum B12 threshold needs to be raised from 200 pg/ml to at least 450 pg/ml because deficiencies begin to appear in the cerebrospinal fluid below 550".
"For brain and nervous system health and prevention of disease in older adults, serum B12 levels should be maintained near or above 1000 pg/ml."
Folate: 29 (8.83-60.8)
Folate is recommended to be at least half way through range (about 35 plus with that range).
It wouldn't hurt to try and improve both B12 and folate by supplementing with a good quality B Complex.
I have used Thorne Basic B for a long time and always been happy. It can go out of stock or become expensive so if you look at different brands then look for the words "bioavailable" or "bioactive" and ensure they contain methylcobalamin (not cyanocobalamin) and methylfolate (not folic acid). Avoid any that contain Vit C as this stops the body from using the B12. Vit C and B12 need to be taken 2 hours apart.
I have recently bought some of this one to try, some other members have found it to be very good. The amounts of the vitamins are very similar to Thorne Basic B, it's liposomal which is said to absorb better, there are no unnecessary added ingredients and better priced:
When taking a B Complex we should leave this off for 3-7 days before any blood test because it contains biotin and this gives false results when biotin is used in the testing procedure (which most labs do).
I was just glancing through StanleyThyroid's post and I noticed they take Centrum advanced 50+ multivitamin and mineral supplement. It appears to contain iodine.
He mentioned that in his reply to SlowDragon which wasn't there when I responded. However, SlowDragon has addressed it, mentioned that we don't recommend multis, pointed out that it contains iodine and given links about why we shouldn't take it
I know it will be a bit of an ‘info mountain’ but work through all the advice and links. This is what I did about 2 years ago. I read for my life and pushed to get onto full replacement dose armed with this knowledge.
When requesting my last dose increase once again I was told by yet another doctor-‘you’re in range’ and I said to that doctor “Yes but there is room in the range for another dose increase and using NICE guidelines I have calculated a guide therapeutic dose of 150ug”.
I had already submitted a printed report with results and references a week earlier for them to chew on. 😂 it‘s all in my bio and on my posts which sit in my profile (click on icons to read people’s journeys).
Could not have done this without support I received from the forum 🤩👍
Well, more energy, more clarity of mind, rarely have heartburn now as I looked at trigger foods which seemed to be certain combinations (all in bio and posts) AND went gluten free (strictly- you can’t be a bit pregnant and you can’t be a bit gluten free ALL or nothing), used to suffer terribly with constipation (much better) well you did ask! 🤣
AND fewer aches and pains - plantar fasciitis disappeared! Went lactofree for a while whist my guts healed, still careful not to hammer dairy. Sleep better, walk farther - for miles not for minutes. I was losing weight but I’ve got my winter tyres on at present- I’ll shake them off in the spring! 😂👍
Taken a while as lost fitness whilst being under medicated (all in bio) and all those years undiagnosed. But the mismanagement early in my diagnosis was the biggest factor by far. My body was starved of thyroid hormone.
It gets better- I hang around as an example and with gratitude for everything this forum has done for me. 🤗
That's really useful. I think many people will be in my situation - newly diagnosed and see little improvement. Its great to know that things can be improved. Having somewhere to talk about the problems is really helpful.
To get the GP to increase your dose of Levo when they are saying , " it's treated now your TSH is in range, go way"
...... put this list under their nose ~ recommendations to keep TSH under about 2/2.5 in patients on Levo and reasons why : healthunlocked.com/thyroidu... my-list-of-references-recommending-gp-s-keep-tsh-
Some are taken straight from GP's resource/ update sites .. one is written by NHS specialist registrars in Cardiology and Endocrinology .. so there should be no argument about their validity .
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")