I've received a letter from Guy's and St Thomas' about the home sleep study I did on 24th October. The letter says I have severe obstructive sleep apnoea. I have a provisional/suspected diagnosis of central hypothyroidism, and also have growth hormone deficiency. I have been titrating up on Levo, starting on 25mcg on 12/09/2022 for 38 days, moving up to 37.5mcg on 20/10/2022 (just 4 days before the sleep test). (I then worked up to 75mcg on 17/11/2022 and will test after 4 weeks as directed by my endo).
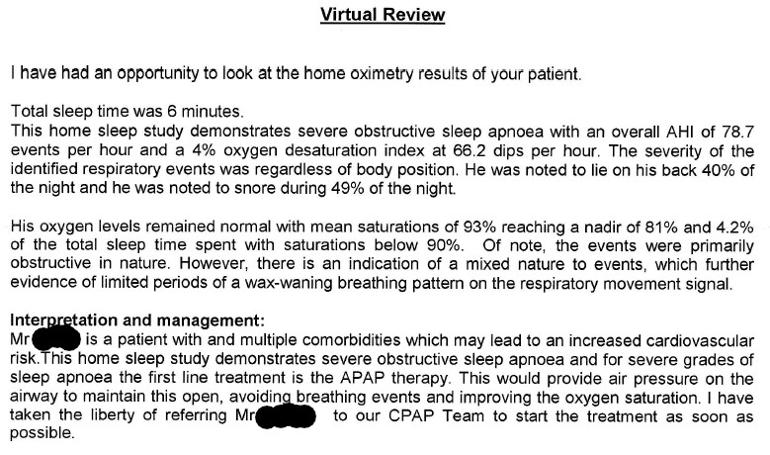
I have attached a screen sot of the main part of the letter, but I have several questions:
The letter days 'Total sleep time was 6 minutes' ... do I take this at face value? I slept for the whole night, and used the machine as instructed. They did call me a couple of weeks ago to arrange for the sleep test to be done, and I told them it had already been done: the person told me they would check if they needed to do it again, and I heard nothing until this letter.
I have read they hypothyroidism can cause sleep apnoea, and I'd already got the connection, and also noted the hypothyroidism symptom of swollen tongue, which I think I have, though it is difficult to know for sure. Is there a direct cause and effect?
Finally, does treatment for hypothyroidism cure/improve the sleep apnoea?
Thanks in advance ...
Written by
UKmale_hypo
To view profiles and participate in discussions please or .
I have hypothyroidism and sleep apnea as well. Along time ago, I read a case study where the apnea improved or disappeared once a patient was optimized on their thyroid meds. I was hoping that my apnea would disappear after I had optimized my levels. It took 20 yrs to get my thyroid levels to improve but unfortunately it didnt take my apnea away. I feel like my tongue size reduced slight from my levels improving but it's still too big for my small mouth.
That said, everyone is different and once your thyroid levels improve it could possibly be a game changer for you. I wonder the 6min is a mistake. How's it possible for them to gather all that info if you slept for 6 minutes only???
I'm currently in the process of getting a MAD. It's been a process since they had it refitted a few times due to my small mouth and how my jaw structure is. I'm cpap non compliant.
Also hoping to get a sleep endoscopy God willingly soon to see where my obstruction is to see if minor procedures could help.
I'll link below 2/3 videos that might be of interest to you. The speaker is Vik Veer and is the top notch sleep ENT and sleep surgeon in the UK. Also will add that there are 2 devices that can help strengthen the tongue. I'm not sure if they are covered in the UK. One is called the Exciteosa and the other is iqoro.com/#
^^^ Vik has a video dedicated to each and their efficacy.
I have both Hashi's and sleep apnoea to name just 2. TBH I don't think there is a single cause of OSA so it would depend what your specific cause is as to whether treatment of hypo will improve it.
I've recently discovered that as I had 4 teeth removed due to overcrowding as a child, my whole bite has changed now over time and may well be the cause of my OSA. I'm getting braces soon to improve my bite but may also need jaw surgery which I am reluctant to do.
It's probably just as easy to resign yourself to using CPAP and do everything you can to make it work for you.
Hi, I've had sleep apnea since developing a goitre. Had sleep study and trialed a cpap but still woke up with mask on. What helps for me is B12- I take 5 squirts methyl B12 sublinguilly daily. Doesn't cure it as still can't sleep on my back, but without it the apnea is chronic.
Folate - 7.8 ug/L (3 - 20) [Sept 2019] I did request in Aug this year
Ferritin - 85 ug/L (25 - 200) [Aug 2022]
B12 - 370 ng/L (200 - 910) [Aug 2022]
Not on any vitamin supplements
Levo dose - yes, I think this needs to increase as I don't feel any better. Am due testing in mid-December. Endo said to start on 75mcg (I stepped up from 25mcg) but I can go up to 125mcg depending on side-effects and FT4 being in upper range.
Brand of Levo: this has been a mess. Was on MERCK, then prescribed TEVA which gave allergic reaction. Now back to MERCK and awaiting new brand.
Many patients do NOT get on well with Teva brand of Levothyroxine.
Teva contains mannitol as a filler, which seems to be possible cause of problems. Teva is the only brand that makes 75mcg tablet. So if avoiding Teva for 75mcg dose ask for 25mcg to add to 50mcg or just extra 50mcg tablets to cut in half
But for some people (usually if lactose intolerant, Teva is by far the best option)
Aristo (currently 100mcg only) is lactose free and mannitol free.
Most easily available (and often most easily tolerated) are Mercury Pharma or Accord
Mercury Pharma make 25mcg, 50mcg and 100mcg tablets
Accord only make 50mcg and 100mcg tablets
Accord is also boxed as Almus via Boots, and Northstar 50mcg and 100mcg via Lloyds ....but Accord doesn’t make 25mcg tablets
If a patient reports persistent symptoms when switching between different levothyroxine tablet formulations, consider consistently prescribing a specific product known to be well tolerated by the patient.
Physicians should: 1) alert patients that preparations may be switched at the pharmacy; 2) encourage patients to ask to remain on the same preparation at every pharmacy refill; and 3) make sure patients understand the need to have their TSH retested and the potential for dosing readjusted every time their LT4 preparation is switched (18).
Netherlands (and Germany?) guidelines are for thyroid patients to always get same brand levothyroxine at each prescription
Levothyroxine is an extremely fussy hormone and should always be taken on an empty stomach and then nothing apart from water for at least an hour after
Many people take Levothyroxine soon after waking, but it may be more convenient and perhaps more effective taken at bedtime
No other medication or supplements at same as Levothyroxine, leave at least 2 hour gap.
Some like iron, calcium, magnesium, HRT, omeprazole or vitamin D should be four hours away
(Time gap doesn't apply to Vitamin D mouth spray)
If you normally take levothyroxine at bedtime/in night ...adjust timings as follows prior to blood test
If testing Monday morning, delay Saturday evening dose levothyroxine until Sunday morning. Delay Sunday evening dose levothyroxine until after blood test on Monday morning. Take Monday evening dose levothyroxine as per normal
Similarly if normally splitting your levothyroxine, take whole daily dose 24 hours before test
Increasing number of members find it smoother/more tolerable to split levothyroxine as two smaller doses, half dose waking, half dose at bedtime.
MERCK was purchased in Spain while I educated my endo on Central Hypothyroidism - they initially refused Levo because they couldn't see it. Then I got TEVA on NHS prescription and got adverse reaction almost immediately, so stopped and back to MERCK. Now waiting on other brand to be delivered.
I've only been waiting for 30 mins before eating or drinking - I will wait an hour from now on.
Any other thoughts about adequate Levo reducing or stopping sleep apnoea?
With serum B12 result below 500, (Or active B12 below 70) recommended to be taking a B12 supplement as well as a B Complex (to balance all the B vitamins) initially for first 2-4 months.
Starting on B12 initially……waiting at least week before adding vitamin B complex
Thorne Basic B recommended vitamin B complex that contains folate, but they are large capsules.
(You can tip powder out if can’t swallow capsule)
IMPORTANT......If you are taking vitamin B complex, or any supplements containing biotin, remember to stop these 7 days before ALL BLOOD TESTS , as biotin can falsely affect test results
In week before blood test, when you stop vitamin B complex, you might want to consider taking a separate methyl folate supplement and continue separate B12
once your serum B12 is over 500 (or Active B12 level has reached 70), stop the B12 and just carry on with the B Complex.
My husbands sleep apnea has resolved on a ketogenic diet and not eating late. Why this has worked, I have no idea, maybe it’s hormonal or maybe it’s eliminated food intolerances. Obviously this won’t necessarily work for everyone but definitely works for him. For years my husband had the worst and loudest snoring you could imagine and awful sleep apnea (I used to keep nudging him to turn onto his side, it’s terrifying!) Sleeping on ones back tends to be really bad for this as it encourages the throat/airways to relax too much and so sewing a tennis ball into the back of ones night shirt can keep a person sleeping on their side through the night. Also, people with sleep apnea should be very careful with certain medications that can cause one to sleep too deeply, inc alcohol and especially stuff like codeine (I read this on one of NHS websites). My Mums cousin was diagnosed with sleep apnea and mysteriously died in her sleep after taking a strong painkiller she’d been given from the hospital after breaking her arm. She was only in her early 60’s and her death came completely out of the blue.
I have had thyroid issues since early 1992 and I did not know that the Hypothyroidism/Hashimotos and Sleep apnea are related. So thank you very much. I do understand the possible airway blockage, that is easy. it is all the other things.
I think they meant 6 hours not 6 minutes. Does 6 hours sound correct from your point of view i.e. what time did you go to bed, how long before you fell asleep then about what time did you wake up. I would bring this error up to them because if makes the whole process foolish if you let this slip. Many of there conclusions are in events per hour, it is widely inaccurate to interpolate into events per hour from readings taken in events per 6 minutes. a bit like taking you pulse for 2 seconds and then concluding that your bpm is 60bpm.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.