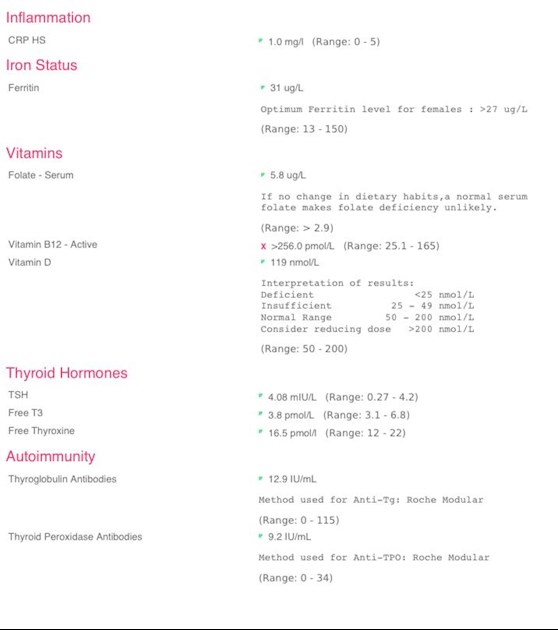
Morning everyone, I should have had a telephone appointment on 23rd of this month with my endo but as usual it’s been cancelled again! However I sent off my October blood results which I had done privately so that he could see that my levels have increased from my previous results. His comeback was that he wants me to stay on 75mcg of Levo! I have told him how I have been feeling via email but his decision is still the same. I will attach my recent results which he insists are within range. Even the report from Medichecks have stated that I am at the high end of the range and need an increase in meds, why do we have this constant battle to change dosage? I am so frustrated .
Increase in Tsh : Morning everyone, I should have... - Thyroid UK
Increase in Tsh
Written by

Kimkat
To view profiles and participate in discussions please or .
Read more about...
14 Replies
•
SeasideSusieRemembering
KimKat
Maybe educate your endo.
TSH should always be no higher than 2 and there is room for it to be much lower - see GP online:
gponline.com/endocrinology-...
Under the section
Cardiovascular changes in hypothyroidism
Replacement therapy with levothyroxine should be initiated in all patients to achieve a TSH level of 0.5-2.0pmol/L.
Also, Dr Toft, past president of the British Thyroid Association and leading endocrinologist, states in Pulse Magazine (the professional publication for doctors):
"The appropriate dose of levothyroxine is that which restores euthyroidism and serum TSH to the lower part of the reference range - 0.2-0.5mU/l. In this case, free thyroxine is likely to be in the upper part of its reference range or even slightly elevated – 18-22pmol/l. Most patients will feel well in that circumstance. But some need a higher dose of levothyroxine to suppress serum TSH and then the serum-free T4 concentration will be elevated at around 24-28pmol/l. This 'exogenous subclinical hyperthyroidism' is not dangerous as long as serum T3 is unequivocally normal – that is, serum total around T3 1.7nmol/l (reference range 1.0-2.2nmol/l).*"
*He confirmed, during a talk he gave to The Thyroid Trust, that this applies to Free T3 as well as Total T3 and this is when on Levo only. You can hear this at 1 hour 19 mins to 1 hour 21 minutes in this video of that talk youtu.be/HYhYAVyKzhw
You can obtain a copy of this article from ThyroidUK:
tukadmin@thyroiduk.org
print it and highlight Question 6 to show your GP.
Also from the British Thyroid Founcation:
btf-thyroid.org/thyroid-fun...
How can blood tests be used to manage thyroid disorders?
.....
Occasionally patients only feel well if the TSH is below normal or suppressed. This is usually not harmful as long as it is not completely undetectable and/or the FT3 is clearly normal.
There are also certain patients who only feel better if the TSH is just above the reference range. Within the limits described above, it is recommended that patients and their supervising doctors set individual targets that are right for their particular circumstances.
Your FT3 is barely in range and this is the active hormone that every cell in our bodies need, this is the result that doctors should be looking at, low FT3 = symptoms. Most of us need FT4 and FT3 fairly well balanced in the upper part of their ranges when on Levo monotherapy.
**
Did you know that your ferritin level is just one point above what the NICE considers iron deficiency - see cks.nice.org.uk/topics/anae...
In all people, a serum ferritin level of less than 30 micrograms/L confirms the diagnosis of iron deficiency.
This wont be helping at all. This level of ferritin and possible iron deficiency will make you feel unwell and no thyroid hormone can work with such a low ferritin level. Some experts say that the optimal ferritin level for thyroid function is 90-110ug/L.
I would ask your doctor to do an iron panel to see if you have iron deficiency and a full blood count to see if you have anaemia. You can have iron deficiency with or witout anaemia. Don't consider self supplementing with iron unless you have an iron panel done and know your serum iron level, too much iron is as bad as too little.
Do you take any supplements? B12 is very high and if you supplement that you don't need to, but your folate level is quite low, it would be better in double figures.
**
Do you always do your thyroid tests as we advise:
* Blood draw no later than 9am. This is because TSH is highest early morning and lowers throughout the day. If looking for a diagnosis of hypothyroidism, an increase in dose of Levo or to avoid a reduction then we need the highest possible TSH
* Nothing to eat or drink except water before the blood draw. This is because eating can lower TSH and coffee can affect TSH.
* If taking thyroid hormone replacement, last dose of Levo should be 24 hours before blood draw, if taking NDT or T3 then last dose should be 8-12 hours before blood draw. Adjust timing the day before if necessary. This avoids measuring hormone levels at their peak after ingestion of hormone replacement. Take your thyroid meds after the blood draw. Taking your dose too close to the blood draw will give false high results, leaving any longer gap will give false low results.
* If you take Biotin or a B Complex containing Biotin (B7), leave this off for 7 days before any blood test. This is because if Biotin is used in the testing procedure it can give false results (most labs use biotin).
These are patient to patient tips which we don't discuss with phlebotomists or doctors.
Thank you SS, lots to read here, I always make sure that I don’t take my Levo before blood draw etc. I was hoping to discuss my vit levels with the endo this time but obviously it’s cancelled. I spoke to secretary who has assured me that she has out all of my concerns into an email to him, in fact I could hear her typing as we were talking. I had already raised certain concerns in my email to him but obviously he knows best 🙄. I’m due to have nhs bloods on the 9th so we shall see what comes of them. My previous Tsh in April was 2.75 and as you see this time it’s 4.75, he didn’t even comment on that so I doubt he even looked at anything else.
SlowDragonAdministrator
Change endocrinologist
Email Thyroid UK for list of recommend thyroid specialist endocrinologists...NHS and Private
tukadmin@thyroiduk.org
The aim of levothyroxine is to increase dose upwards in 25mcg steps until TSH is ALWAYS under 2
When adequately treated, TSH will often be well below one.
Most important results are ALWAYS Ft3 followed by Ft4.
When adequately treated Ft4 is usually in top third of range and Ft3 at least 60% through range (regardless of how low TSH is)
Extremely important to have optimal vitamin levels too as this helps reduce symptoms and improve how levothyroxine works
Ferritin level is terrible
Look at increasing iron rich foods in diet
GP should do full iron panel test for anaemia
cks.nice.org.uk/topics/anae...
In all people, a serum ferritin level of less than 30 micrograms/L confirms the diagnosis of iron deficiency
Look at increasing iron rich foods in diet
Eating iron rich foods like liver or liver pate once a week plus other red meat, pumpkin seeds and dark chocolate, plus daily orange juice or other vitamin C rich drink can help improve iron absorption
List of iron rich foods
Links about iron and ferritin
irondisorders.org/too-littl...
davidg170.sg-host.com/wp-co...
Great in-depth article on low ferritin
oatext.com/iron-deficiency-...
drhedberg.com/ferritin-hypo...
This is interesting because I have noticed that many patients with Hashimoto’s disease and hypothyroidism, start to feel worse when their ferritin drops below 80 and usually there is hair loss when it drops below 50.
Thyroid disease is as much about optimising vitamins as thyroid hormones
healthunlocked.com/thyroidu...
restartmed.com/hypothyroidi...
Post discussing just how long it can take to raise low ferritin
healthunlocked.com/thyroidu...
Never supplement iron without doing full iron panel test for anaemia first
Iron and thyroid link
healthunlocked.com/thyroidu...
Posts discussing why important to do full iron panel test
healthunlocked.com/thyroidu...
healthunlocked.com/thyroidu...
Folate is poor
What vitamin supplements are you currently taking
Approx how much do you weigh in kilo
My weight is around 68 kilos, I take vit C, VitD & K2 and B12. I also take collagen for hair nails etc. my diet is good and I include liver/pate etc. As I said to seaside Susie I was hoping to discuss this with my endo but that’s not to be now. I have sent an email to TUK for a list of endocrinologists as I am rapidly losing my patience with this guy, I don’t think he really read my email that accompanied my October bloods, which doesn’t surprise me. Thank you for the info above.
guidelines on dose levothyroxine by weight
Even if we frequently don’t start on full replacement dose, most people need to increase levothyroxine dose slowly upwards in 25mcg steps (retesting 6-8 weeks after each increase) until eventually on, or near full replacement dose
NICE guidelines on full replacement dose
nice.org.uk/guidance/ng145/...
1.3.6
Consider starting levothyroxine at a dosage of 1.6 micrograms per kilogram of body weight per day (rounded to the nearest 25 micrograms) for adults under 65 with primary hypothyroidism and no history of cardiovascular disease.
Also here
cks.nice.org.uk/topics/hypo...
gp-update.co.uk/Latest-Upda...
Traditionally we have tended to start patients on a low dose of levothyroxine and titrate it up over a period of months. RCT evidence suggests that for the majority of patients this is not necessary and may waste resources.
For patients aged >60y or with ischaemic heart disease, start levothyroxine at 25–50μg daily and titrate up every 3 to 6 weeks as tolerated.
For ALL other patients start at full replacement dose. For most this will equate to 1.6 μg/kg/day (approximately 100μg for a 60kg woman and 125μg for a 75kg man).
If you are starting treatment for subclinical hypothyroidism, this article advises starting at a dose close to the full treatment dose on the basis that it is difficult to assess symptom response unless a therapeutic dose has been trialled.
BMJ also clear on dose required
68 kilo x 1.6mcg = 108.8mcg levothyroxine per day as the likely dose levothyroxine required
That’s approx 100mcg 3 x week and 112.5mcg 4 x week
Request endocrinologist increase levothyroxine by 25mcg as per guidelines and retest in 6-8 weeks
Just to show you what I am working with, I will add the email from my endos secretary that I have just read, this was about an hour after we spoke this morning
Have removed image as contained Dr details
Sorry I’ll try to erase it.
This should be ok
Black and white
Write back and include links to guidelines on dose by weight and that on levothyroxine TSH should always be under 2
Request 25mcg dose increase in levothyroxine as per guidelines
Include recent Medichecks results and tick list of current hypothyroid symptoms.
(Tick all that apply)
thyroiduk.org/wp-content/up...
Yes thanks again slow dragon, I did include recent bloods which he claims are within range, even though they are higher than last time. I had already sent him the checklist, which I think made him a little agitated and he told me that he could decipher results thank you! This was on my last appointment six months ago. I really think that I’ll just try and change my consultant as hd obviously isn’t taking any notice of my concerns. I’ll put another email together tomorrow though and see how that goes down,
NHS England Liothyronine guidelines July 2019 clearly state on page 13 that TSH should be between 0.4-1.5 when OPTIMALLY treated with just LevothyroxineNote that it says test should be in morning BEFORE taking levothyroxine
Also to test vitamin D, folate, B12 and ferritin
sps.nhs.uk/wp-content/uploa...
Graph showing TSH in healthy population
web.archive.org/web/2004060...
Aim is to bring a TSH under 2.5
UK guidance suggests aiming for a TSH of 0.5–2.5
SlowDragonAdministrator
Also point out that you have very low ferritin and that you are likely anaemic
Hello Kimkat :
Well I think at this pint in time you need to start rethinking the respect you likely still hold for this endocrinologist.
Your Ferritin is way too low to assist your body in converting the 4 - Levothyroxine.
Has your ferritin been investigated and are you now taking supplements as everywhere I read ferritin needs to be over 70 for any thyroid hormone replacement to work :
Your TSH is too high for someone on thyroid medication and your T3 and T4 too low to help restore your health and well being.
A fully functioning working thyroid would be supporting you daily with trace elements of T1. T2 and calcitonin plus a measure of T3 at around 10 mcg plus a measure of T4 at around 100 mcg.
T4 needs to convert within your body into T3 and T3 is said to be around 4 times more powerful than T4 with the average person needing to convert and utilise around 50 T3 daily just to function.
Your body needs optimal ferritin, folate, B12 and vitamin D to assist in this process of conversion.
RAI is known to trash vitamins and minerals :
Primary hypothyroidism caused by RAI is know to be more difficult to treat :
Some people can get by on T4 only, some people find that at some point in time T4 seems to not work as well as it did and need to add a little T3 with their T4 making a T3/T4 combo : some people can't tolerate T4 and ned to take T3 only : whilst other people prefer to take Natural Desiccated Thyroid.
You have lost your thyroid and by not replacing your own T3 thyroid hormone production you have in effect been down regulated by some 20% of your overall well being and given time that will pull you down even further.
Your thyroid was a major gland responsible for full body synchronisation including your physical, mental, emotional, psychological and spiritual well being, your inner central heating system and your metabolism.
I became very unwell some 8 years after ingesting RAI in 2005 and " seen " as a conundrum by my doctor and I was refused any treatment option by T4 - Levothyroxine monotherapy.
I know self medicate and have my life back :
I trialled a little T3 with my T4 and it was just like that light bulb moment we read about - and my brain felt like it had been turned on :
I then trialled Natural Desiccated Thyroid and found this " softer " on my body and have been very happy on this " original " of all thyroid hormone replacements for the past 4 years and just take a yearly blood test more to see where my vitamins and minerals are, than where my T3 sits - as I still need to supplement ferritin, folate, B12 and vitamin D :
Not what you're looking for?
You may also like...
TSH 65
Hi everyone,
I was diagnosed 10 years ago as hypothyroid, and was on 175mcg Levo. Before this I had...
Increase in TSH.
Hi all.
After increasing my levo from 75mcg to 100mcg in mid/late 2016 it caused me problems and my...
Been given a reluctant temporary increase in meds
I posted the other day about being under medicated. TSH 4.91 (0.46 - 5) T4 12.2 (12 - 22) T3 1 (0.9...
Sudden increase in TSH
Hi
I've been on a dose of 100mcg for about 8 years - male 51, 90kg. I did have an increase in dose...
Severe Depression with TSH at 4.02
I am so grateful for the posts this week helping with my own hypothyroidism diagnosis.
I have also...