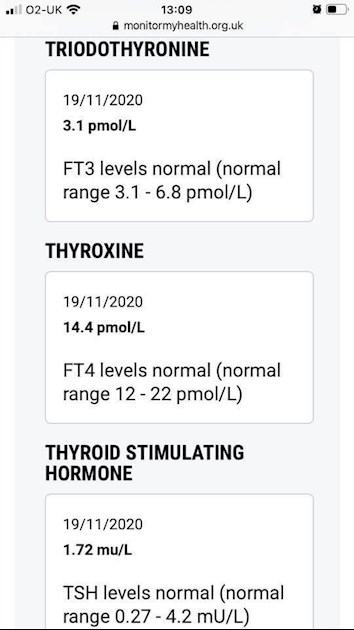
I have ME/CFS, fibromyalgia, pernicious aneamia etc but I have all the symptoms of hypothyroidism. My FT3 & FT4 were the very low end of normal and my TSH seems normal. I also started taking LDN a little over a month before. Is it possible that I have a thyroid issue and that the LDN has impacted the test?
Written by
Jdizz7
To view profiles and participate in discussions please or .
Don't know anything about LDN, I wouldn't have thought it would affect thyroid hormone levels.
Your TSH is way too low for your low normal fT3 AND ft4. Normally when fT4 starts to fall TSH rises dramatically and this preserves average fT3 levels. The TSH stimulates the thyroid to work harder and stimulates T4 to T3 conversion, particularly the type of conversion which maintains cellular T3 levels. This dramatic rise in TSH makes it an excellent marker for primary hypothyroidism - a failing thyroid gland.
In your case your pituitary isn't responding adequately. This isn't really 'secondary hypothyroidism' which is usually associated with a damaged pituitary, it is a more subtle form which I call subnormal TSH secretion. This can have profound effects because not only do you have lower fT3 AND fT4 than normal but also you get reduced T4 to T3 conversion in tissues such as the brain and skeletal muscles that rely on the TSH stimulus. Unfortunately, endocrinologists fail to work this out and don't recognise this form of hypothyrodism.
Subnormal TSH secretion can be caused by a period of thyrotoxicity which 'down-regulates the hypothalamic pituity thyroid axis'. This can occur after a period of thyrotoxicosis, overactive thyroid, which you may not notice. It can also be caused by very strict dieting, depression or a concurrent severe illness. Ideally you would identify and correct the underlying cause but in practice the only way forward is to take thyroid hormone usally with some T3 in the form of liothyronine or NDT.
CFS/ME and fibromyalgia are 'new' diseases that were identified after endocrinologists started (mis)using thyroid blood tests for diagnosis, rather than going by signs and symptoms. I would strongly urge you to push hard for a trial of thyroid hormone, it will be very difficult to persuade a doctor but give it your best shot.
Is it not possible that the LDN has caused secondary hypo (despite its anti-immune properties)? Ive read that Central hypo may be induced by inhibition of thyroid-stimulating hormone (via bexarotene or corticosteroids) or by immunological mechanisms (via anti-CTLA4 or anti-PD-1 antibody drugs) plus other drug effects but is the full list known?. pubmed.ncbi.nlm.nih.gov/199...
Personally I believe that my own thyroid symptoms/test results are caused by a prescription drug not (yet) "on the list" that disrupts the HPTA axis.
Alternatively maybe such unidentified drugs may exacerbate 'hypothyroidism' in patients with non-thyroidal illness" a la rexinoids? researchgate.net/publicatio...
Hi ME/CFS and fibromyalgia are not “new” diseases. I don’t doubt that there are patients wrongly diagnosed that have thyroid issues or other issues altogether. However there is plenty of medical evidence available to show that ME is an illness different to low thyroid. If you’re interested I’d suggest reading up on Dr Ron Davis and Bhupesh Prusty’s work or Jennifer Brea.I do appreciate your advice and suggestions and will speak to my GP.
LDN is used to help block the opioid receptors and the immune system.
By 'new' I mean their incidence increased dramatically as diagnosis and treatment of hypothyrodism switched from diagnosis based on signs and symptoms and treatment with levothyroxine monotherapy instead of NDT. This occurred during the 1970s as accurate TSH assays became available. So, 'new' is quite old in this context.
The late Dr John Lowe found a high proportion of his fibromyalgia patients responded to his 'metabolic rehabilitation' therapy. This was not just treatment of hypothyroidism with liothyronine, it involved other approaches such as exercise to tolerance (not to exhaustion!). I've no doubt Dr Lowe's approach was effective but we have to be careful about extrapolating his numbers to the general fibromyalgia population. Patients are very good at self diagnosis and I suspect those patients who found they 'clicked' with his list of signs and symptoms went to see him and got better. Those who didn't recognise his description of signs and symptoms would have gone elsewhere. So, we don't know what percentage of the fibromyalgia community would benefit from liothyronine therapy.
Purely from a thyroid viewpoint your fT3 and fT4 are abnormal. When fT4 is not high or in the upper half of its reference interval, TSH is usually high enough to stimulate sufficient T4 to T3 conversion to maintain average fT3 levels. This is done by type-2 deiodinase (D2) which takes place in organs such as the brain and skeletal muscles. D2 controls local T3 levels. Although we cannont measure tissue T3 levels we can logically deduce that tissues dependent upon D2 for adequate local T3 are likely to be hypothyroid if both fT3 and fT4 are low normal. This low normal fT3 indicates there is reduced D2 activity and hence reduced local T3 in D2 regulated tissues.
Organs such as the brain take in mainly T4 and use D2 to regulate T3. If D2 activity is too low (because of insufficient stimulation from TSH) then restoring normal serum fT3 will not be adequate - because the brain (and skeletal muscles) want to take in T4 not T3. In this situation you need to hope that TSH secretion returns to normal or take sufficient liothyronine to resolve the hypothyroid signs and symptoms. However, this amount of liothyronine may push fT3 high and be too high for those tissues that do not express D2 and so take T3 direct from the blood. To some extent the heart does this, it has some D2 activity but not a lot. So, there may be an uncomfortable compromise between taking liothyronine to resolve symptoms but not so much that there are signs of too much.
Have you had nutrients tested......vit D, vit B12, folate and ferritin need to be optimal in order to support thyroid function.
I too was diagnosed with CFS/ME and fibromyalgia but was never convinced that my problems lay there....so I started "digging". I already had a diagnosis of hypothyroidism but after taking increasing doses of levothyroxine for20 years I ended up barely able to function. Low cellular T3 turned out to be my problem
Research has shown that some FM patients suffer from lowT3
Your thyroid is not producing enoughT4....your FT4 is only 24% through the reference range when it should be approaching 75%
Your conversion may be poor but until FT4 is raised and we see how that affects FT3 labs(which needs to be tested....it is the important reading!) it's difficult to be certain.
High FT4 with low FT3 indicates poor conversion.
I know nothing about LDN but it probably has no impact on thyroid tests, this might help....
I suggest that first you need levothyroxine and that you also need to optimise the nutrients ( above).
Based on your symptoms and low FT4 ask your GP to give you a trial with levothyroxine, asking for a trial first might be viewed more favourably by a GP that just asking straight out for the hormone.....many of them don't like to feel their authority is being undermined by a patient. Been there!
You should be given 50mcg as a starter dose to be tested 6/8 weeks later and the dose increased as required. You will eventually need more than 50mcg! Retest and increase until FT4 is raised sufficiently and symptoms ease.
If this doesn't really help then you may need to add T3 but it's best to work through one stage at a time. Been there too!
Since your TSH is at a reasonable level for someone not taking levo you will need to put forward a convincing case for levo. GPs tend to view the TSH test as the gold standard test when they should, after diagnosis, be focusing on FT4 and FT3. Suggest you write down all the things you want to say to your GP and take this to consultations.....I found that stopped me rambling on and sounding confused.
Fibromyalgia is often undiagnosed hypothyroid especially autoimmune thyroid disease also called Hashimoto’s
For full Thyroid evaluation you need TSH, FT4 and FT3 plus both TPO and TG thyroid antibodies tested. Also EXTREMELY important to test vitamin D, folate, ferritin and B12
Low vitamin levels are extremely common, especially if you have autoimmune thyroid disease (Hashimoto's) diagnosed by raised Thyroid antibodies
Ask GP to test vitamin levels and thyroid antibodies
Recommended on here that all thyroid blood tests should ideally be done as early as possible in morning and before eating or drinking anything other than water .
This gives highest TSH, lowest FT4 and most consistent results. (Patient to patient tip)
Private tests are available as NHS currently rarely tests Ft3 or thyroid antibodies or all relevant vitamins
If TPO or TG thyroid antibodies are high this is usually due to Hashimoto’s (commonly known in UK as autoimmune thyroid disease).
About 90% of all primary hypothyroidism in Uk is due to Hashimoto’s. Low vitamin levels are particularly common with Hashimoto’s. Gluten intolerance is often a hidden issue to.
Hi I these results were from monitor my health. Unfortunately the vit d test failed twice. However due to secondary hyper parathyroidism which the GP believed was due to low vit D that I had roughly 10 years ago and living in Scotland I take a vit d supplement.I was diagnosed with pernicious aneamia roughly 10 years ago too, which for me is autoimmune and hereditary. My immune system attacks the intrinsic factor which is needed to absorb b12-treatment is B12 injections. Due to heavy menstruation (since they started) I have also been given ferritin and I take a folate supplement.
I am always a bit cautious about such claims. For example, does the author mean that TSH is reduced? Or that Free T4 is increased? Or that Free T3 is increased? Or some other combination of these?
To me, the only thing that matters with substances like LDN or perhaps a new supplement is whether or not it is safe for me personally, and whether or not it makes me feel better.
The other issue, of course, is whether any change in Thyroid Function Test results as a result of taking LDN or new supplements actually lead to my prescribed thyroid hormones being inappropriately reduced.
When a patient is at her optimal LDN dose, lab results will begin to manifest with decreased thyroid markers (i.e. TSH, T4, T3, and TPO levels)
Decreasing all four of TSH, T4, T3 and TPO doesn't like like good news to me.
If Free T4 and Free T3 increase then I would expect TSH to reduce. If Free T4 and Free T3 decrease then I would expect TSH to increase.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.