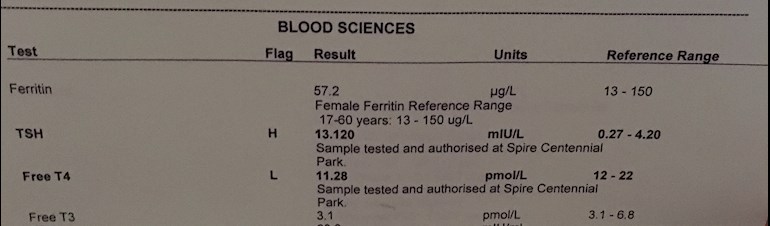
So I have received results from private tests based on which, my dose of Levo has been doubled from 50 to 100mgs. I go back in 6 weeks for retesting, any thoughts on the other results?
Test results: So I have received results from... - Thyroid UK
Test results
Written by

Kip4
To view profiles and participate in discussions please or .
Read more about...
11 Replies
•
SlowDragonAdministrator
Levothyroxine dose is usually only increased in 25mcg steps and retesting in 6-8 weeks
Then dose increased again if necessary.
Increasing too quickly can be hard to tolerate. But you may sail through
See how you get on, but if you find it too much, you could reduce to 75mcg for few days/weeks
Many people find Levothyroxine brands are not interchangeable.
Once you find a brand that suits you, best to make sure to only get that one at each prescription. Watch out for brand change when dose is increased or at repeat prescription.
Many patients do NOT get on well with Teva brand of Levothyroxine. Though it is the only one for lactose intolerant patients
Ask GP to test vitamin D, folate and B12. These are often too low when we have been under medicated.
Have you ever had TPO and TG thyroid antibodies tested to see if cause of hypothyroidism is due to autoimmune thyroid disease also called Hashimoto's
Ask for testing if never been done
About 80-90% of all hypothyroidism in Uk is due to Hashimoto's. Low vitamins are especially common with Hashimoto's. Food intolerances are very common too, especially gluten. So it's important to get TPO and TG thyroid antibodies tested at least once .
NICE guidelines saying how to initiate and increase. Note that most patients eventually need somewhere between 100mcg and 200mcg Levothyroxine
cks.nice.org.uk/hypothyroid...
I had all tested, I couldn’t attach more than one photo though, or couldn't work out how to !! I’ll post two more pics with the other results
You can only add one picture per post
I tried the link to Guidelines, but got a page saying "Unfortunately this site is only available from Great Britain." Any idea how someone in the U.S. can see these guidelines?
The NICE website will only be available from UK as it's a UK organisation
Here's the relevant section
Initiation and titration
The dose of levothyroxine (LT4) should be individualized on the basis of clinical and biochemical (thyroid function tests) response.
Treatment must be monitored regularly to determine an adequate dose and to avoid both under-treatment and over-treatment.
The initial recommended dose is:
For most people: 50–100 micrograms once daily, preferably taken at least 30 minutes before breakfast, caffeine-containing liquids (such as coffee or tea), or other drugs.
This should be adjusted in increments of 25–50 micrograms every 3–4 weeks according to response.
The usual maintenance dose is 100–200 micrograms once daily.
For people aged over 50 years and people with cardiac disease or severe hypothyroidism: 25 micrograms once daily, adjusted in increments of 25 micrograms every 4 weeks according to response.
Once a stable thyroid-stimulating hormone (TSH) level is achieved and an adequate dose determined, arrange follow up to check thyroid function tests (TFTs) at 4–6 months and then annually.
Is there anything in the guidelines about adding T3 to the treatment?
No currently NHS and NICE deny we need any at all!
Thank you!
There are recent articles in the U.S. National Institutes of Health database (Pub Med) on therapy that includes T3 and dangers of low T3 levels.
1. On why some doctors are adding T3: ncbi.nlm.nih.gov/pubmed/302...
2. On the shortcomings of monotherapy (T4 only): ncbi.nlm.nih.gov/pubmed/299...
3. On superiority of supplying both T4 and T3: ncbi.nlm.nih.gov/pubmed/298...
And the effects of low T3
1. Alzheimer's risk: ncbi.nlm.nih.gov/pubmed/302...
2, Diabetic neuropathy: ncbi.nlm.nih.gov/pubmed/302...
3. Cholesterol lowering effectiveness of statins: ncbi.nlm.nih.gov/pubmed/299...
There were 8,336 results when I searched on "triiodothyronine thyroid treatment " on ncbi.nlm.nih.gov/pubmed I hope there are some medical folks, researchers, etc. out there who see this.
Thanks I shall have a good read
Many of us long term "difficult patients" who have moaned that Levothyroxine on its own doesn't work....turn out to have DNA issues
Getting DIO2 gene test can help medics accept you might need some T3
But often "out of date" medics just treat you like a drug addict, for taking T3 or that it's just a placebo
Though how a placebo can give the difference between not being mobile and returning to normal life......they have yet to explain!
My own GP initially said "you can't take that, it will kill you" ......but having now seen my transformation after a year on T3, is fully supportive
Thanks Slow Dragon for your help again, maybe it’s the placebo effect but since dose change last Friday, I am sleeping much better. Let’s see how it goes, however small steps I appreciate! 😊
Not what you're looking for?
You may also like...
Test results
Hello, can anyone advice on the following results? I have my ferritin, folate and B12 results...
Test results
Just spoke to doc about results: they didn't check my free t3 and t4 it was a gamble they would....
Test results
I've just received blood my test results from monitor my health. I've got moderate/severe me/cfs...
test results
my test results have come back abnormal the GP had been tweaking my levothyroxine for over 6 months...
Test results
Hi all,
Was wondering if anyone could offer advice on my latest test results?
I was also being...