On the one hand, we keep getting told that medics know exactly how to get our doses right. Simple, isn't it? And "they" know all about how it works. (Sorry - can't be bothered to carry on with the usual stuff we all know.)
On the other hand we read an abstract which is able to say:
"... each H [hypothalamus] P [pituitary] characteristic curve being uniquely defined for each individual akin to a fingerprint..."
In case you do not know who "Dietrich JW" is, have a look here:
thyroiduk.org.uk/tuk/About_...
")
Math Biosci. 2014 Jan 27. pii: S0025-5564(14)00006-6. doi: 10.1016/j.mbs.2014.01.001. [Epub ahead of print]
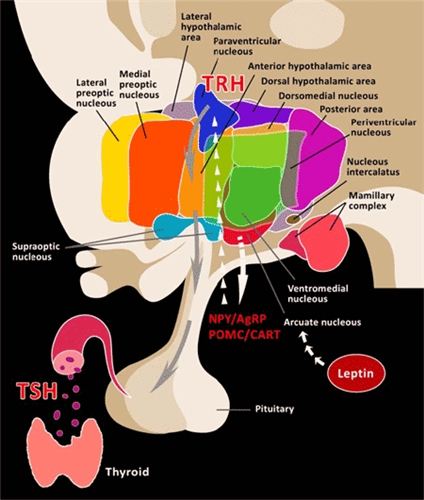
A Novel Minimal Mathematical Model of the Hypothalamus-Pituitary-Thyroid Axis Validated for Individualized Clinical Applications.
Goede SL1, Leow MK2, Smit JW3, Dietrich JW4.
Author information
1Electronic Engineering, Private Research and Consultancy Oterlekerweg 4, 1841 GP Stompetoren, The Netherlands. Electronic address: slgoede@kpnmail.nl.
2Singapore Institute for Clinical Sciences, Brenner Centre for Molecular Medicine, A∗STAR; Tan Tock Seng Hospital; National University of Singapore; Duke-NUS Graduate Medical School Singapore. Electronic address: melvin_leow@nuhs.edu.sg.
3Department of General Internal Medicine of Radboud University Nijmegen Medical Centre, Postbus 9101, 6500 HB Nijmegen, The Netherlands. Electronic address: j.smit@aig.umcn.nl.
4Laboratory XU44; Medical Hospital I Bergmannsheil University Hospitals Ruhr University of Bochum D-44789 Bochum, NRW, Germany. Electronic address: johannes.dietrich@ruhr-uni-bochum.de.
Abstract
The hypothalamus-pituitary-thyroid (HPT) axis represents a complex, non-linear thyroid hormone system in vertebrates governed by numerous variables. The common modeling approach until now aims at a comprehensive inclusion of all known physiological influences. In contrast, we develop a parsimonious mathematical model that integrates the hypothalamus-pituitary (HP) complex as an endocrinologic unit based on a parameterized negative exponential function between free thyroxine (FT4) as stimulus and thyrotropin (thyroid stimulating hormone, TSH) as response. Model validation with clinical data obtained from geographically different hospitals revealed a goodness-of-fit largely ranging between 90% <R2 < 99%, each HP characteristic curve being uniquely defined for each individual akin to a fingerprint. Specifically, the HP model represents the afferent feedback limb of the HPT axis while the efferent limb is mathematically depicted by TSH input to the thyroid gland which responds by secreting T4 as its chief output. The complete HPT axis thus forms a closed loop system with negative feedback resulting in an equilibrium state or homeostasis under defined conditions illustrated by the intersection of the HP and thyroid response characteristics. In this treatise, we demonstrate how this mathematical approach facilitates homeostatic set points computation for personalized dosing of thyroid medications of patients to individualized euthyroid states.
Copyright © 2014. Published by Elsevier Inc.
KEYWORDS:
Clinical validation, Individualized therapeutic target, Logarithmic-linear relationship, Negative exponential, Parameterization
PMID: 24480737 [PubMed - as supplied by publisher]
ncbi.nlm.nih.gov/pubmed/244...
Rod
