Just found this "detox" advice on a RLS Facebook page I was looking through.
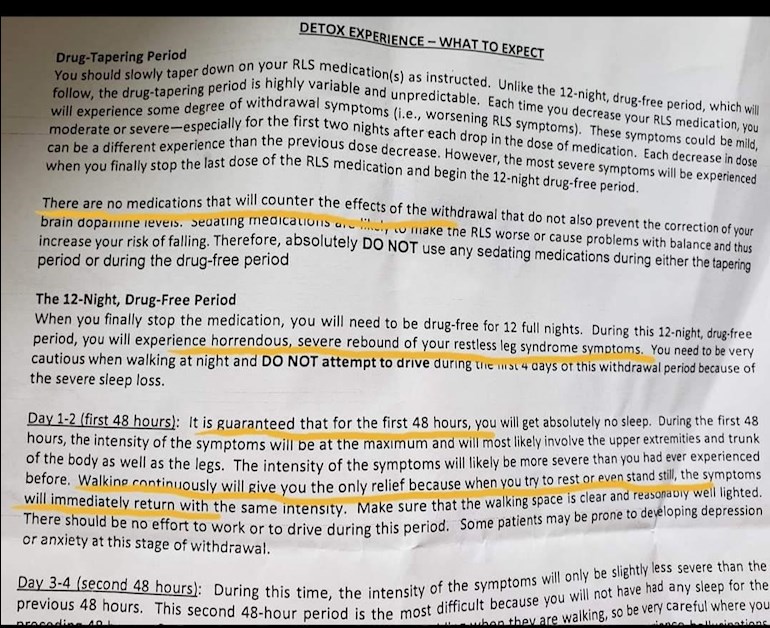
It's the first time I've ever seen a formal sheet explaining what will happen during DA withdrawal.
It certainly reflects what I went through. It might be useful for anyone going through it, or thinking of doing so. It would perhaps persuade GPs how horrendous withdrawal from Ropinirole and Pramipexole is for the vast majority.
It talks about a 12 day drug free period so I suspect it's from Dr Christopher Earley at Johns Hopkins University Hospital in Baltimore, USA who favours the drug free washout period to establish the base level of your RLS.
Written by
Joolsg
To view profiles and participate in discussions please or .
A patient of dr Earley here on HU mentioned that he usually advised a completely drug-free period. Thus stopping the DA promptly without anything to replace it. I have no idea whether dr Earley still favours or advocates this approach. Does someone know?
It is Dr. Earley's advice sheet.I found it useful because it clearly sets out how horrendous it will be. If I had been able to show this to my GP after 4 days of zero sleep, she may have believed me and not treated me like a pathetic whinging woman.
Hopefully someone going through DA withdrawal can show it to their GP when begging for opioids to help them through it.
I went through it for 5 days. I finally had to go back on the Neupro. My Dr totally abandoned me. Refused to prescribe methadone told me to just find a pain management Dr. I almost jumped off my apartment building. I had no idea what was wrong with me or why my body was shaking I fell multiple times. It was the worst week of my life. These DAS ARE EVIL.
I'm so sorry to hear that. The only way to get off these drugs is with a lot of support from our doctors. Sadly, that just doesn't happen.
I'm lucky that I found a GP willing to prescribe buprenorphine on a 3 week trial. It worked completely and she continued the prescription. I live in dread that it will be stopped.
Low dose opioids are the only drugs that work for many of us after DAs.
One day, the medical profession will hang its head in shame over the treatment of RLS patients. We are gaslit, treated as drug seeking hypochondriacs and left to fight for help. The disease is regarded as a minor irritation.
I only have experience in coming off opiates ( fentanyl) . It took me 18 months to get from over 70 to zero. The final 10 days I used valium and Clonidine.I certainly could not envisage going cold turkey. It was quite awful enough going through the very slow taper.
I got absolutely no help from the medical profession, apart from bullying my GP to prescribe the Valium and Clonidine.
The drug free period described above should really be only done in a medically supervised situation.
I agree. My neurologist…or former neurologist I should say from John’s Hopkins’s took me off Neupro cold turkey. It took me 5 days to start thinking about killing myself. I’m not joking. I wouldn’t advise Anyone to try to come off this dangerous drug cold turkey. It was the worst experience of my life. Please be careful.
Because I see that you mentioned Tramadol I just wanted to say that if you're still taking it and don't know that Tramadol also can cause augmentation. I was on it for over 10 years before I figured out, from another RLS forum, the reason my RLS got so bad was because of the Tramadol. I got up to taking the mass dose per day (400mg). I'm currently complete off the Tramadol and now taking Methadone and my RLS has improved tremendously. I just wanted to make sure you knew, just in case.
I only used Tramadol during withdrawal and knew about augmentation. I was put on Oxycontin and it's not brilliant.Getting methadone here in the UK is impossible. Our doctors and neurologists aren't taught about RLS at any stage during training and the few neurologists who know something about RLS are at least a decade behind the top US experts on medications.
I've been in an email argument with the top UK specialist trying to get Buprenorphine. He eventually conceded that he had no objection to Buprenorphine BUT he wouldn't prescribe it. I would have to persuade my GP to do that. It will be very difficult but I'm going to push.
Ah that's what I thought.I'm on 6x5 Oxynorm which works fine. Not keen on 4 hourly med but I found the slow release only lasted 8 or so hours. Thank goodness I have it though. What do you find your triggers are?
I think he means sedating. I remember when going through withdrawal I used diazepam and it gave me a drugged up feeling and I fell over badly at least 3 times. I was at the stage where walking was the only thing that stopped the horrendous all over body RLS but I was too exhausted by lack of sleep and MS so the sedatives made it worse.
I wonder does he mean so called sleeping tablets such as zopiclone? If so, I would agree that they should be avoided. They make everything worse when RLS symptoms are through the roof.
I am on the last leg from 2MG daily over 3 months ago - now on 250 MCG daily, so through , what I thought, was the worst patch but maybe not? Sounds like the final drop will be the worst - any experience out there before I make the leap?
I found that cannabis was the only thing that helped in the 6 days after dropping the last dose.I think the vast majority will experience the hell described by Dr Earley ( I did) but some people manage with minimal suffering.
Make sure you take time off work and have someone to help. My husband stayed up with me as I was very unstable and did honestly consider throwing myself out of the window.
I used tramadol 50mg every 4 hours during the week after the last dose of Ropinirole and smoked cannabis which gave me 30 minutes of desperately needed sleep.
My GP was APPALLING. She thought I was 'hysterical' and actually told me to drink milk for the calcium!!
Luckily my MS neurologist answered my calls and told the GP to give me tramadol as needed and Oxycontin for replacement treatment.
Targinact should help. It may be worth trying to build up a stash so that you can slightly increase the dose during the worst days immediately after the last tablet (though obviously taking care to avoid an opioid overdose which is not recommended). I definitely notice that people who take it VERY gradually report slightly less severe symptoms than those who rush it. Also, there is some evidence to suggest that keeping serum ferritin high during the withdrawal helps avoid the very worst symptoms.
i think many people have reported a similar effect. Certainly my 25mg of oxycontin is no longer working as effectively. i suspect we will have to switch to another opioid which might work in a slightly different way and affect different receptors. just wish we could get low dose methadone, like our US friends.
thank you for posting this! I too would like to see the full article or the Facebook page you obtained this from. I tried to Google it just to realize that it's like searching for John Doe.
I found it yesterday while looking through a facebook group called Restless Legs Syndrome ( worldwide support group). The post is below and the poster confirmed it's from Dr. Earley at Johns Hopkins.
I live in Baltimore and had a consult with Dr. Earley recently where I received this exact information in person. It freaked me out completely. I appreciate the "straight talk" here, but I'm so scared to begin the process!
It's brutal and you think you'll never make it. But many have done it and survived. Once off Ropinirole/Pramipexole the RLS reduces in severity. Hopefully new meds will give complete cover.Best of luck. I wish you strength.
Thank you! I've been reading many posts here and it seems like lowering inn extremely slow increments is the way to go? I contacted a compounding pharmacy that can make Mirapex into tiny doses. Does this sound right?
I read a post by someone who did this and reduced by tiny, tiny amounts over a year while increasing the alternative med.It sounds very sensible and I wish I'd known about it!
Ensure you raise your serum ferritin above 100 ( some need it above 300). You may even be someone who can be med free.
I have an orange. RLS defined is an apple. Day time awakened jerks, more Fractured Myoclonic movement disorder(Not exact) but better discription than sleep disorder. So Augmentation is not the issue but really what is it and what to change if the meds are working for an orange?
Just for clarification. Based on previous exchanges with Bill, he is comparing RLS with myoclonus and is saying that these two conditions are unrelated, just as apples and oranges are. He has written that RLS is the apple and myoclonus is the orange.
He writes that he has daytime involuntary movements due to myoclonus. This is not a sleep disorder, because it happens during the day. RLS is presumably a sleep disorder, it happens at night.
Bill doesn't think he has daytime symptoms because of augmentation, but because he has myoclonus.
He thinks that his myoclonus is a variant not described before.
He does take RLS meds, but seems to be saying that they work for his myoclonus.
Thank you so much for this, Jools. As others have commented, it provides independent verification (when so often we were dismissed as over-dramatising and sensitive) of the torture that we experienced coming off these vicious drugs.
I did a bit of research to see if I could track down the document. The website of the JohnsHopkinsUniversityHospital, where Dr. Earley works, has some useful information and webinars about RLS but the document was not available publicly.
However, I did uncover something which is somewhat tangentially relevant. The widow of Robin Williams (the actor) suspects that his suicide may have been linked to a change in dopamine agonist medication which occurred shortly before his death when he was prescribed sinemet in place of pramipexole - n.neurology.org/content/lew...
Robin Williams was suffering from a form of dementia (Lewy body dementia) which was misdiagnosed as Parkinsons and in consequence he was unnecessarily being treated with dopamine agonists. It served to increase my anger about these drugs - so often mis-prescribed by the medical profession - may have contributed to the loss of Robin Williams so unnecessarily early.
I didn't know that. I live in hope that these drugs will be monitored far more closely. The doctors prescribing them don't have enough knowledge or information about RLS or DAs to monitor patients safely.
Hi , I wonder if you a full version of the detox page you posted9 mths as it finished on day 4 of 12 …I’m presently 20 days from starting that 12 day countdown.. something to look forward to…thanks
Sadly not as it was copied from a FB page.However, rls.org have a detailed schedule in their member's section and I think it has the full schedule.
Basically, days 1-4 are hell on earth, then you start to get 30 mins to an hour rest each day until day 7. After that, you get an hour or two sleep and the symptoms start to ease.
That schedule is the drug free withdrawal. Many get opioids and cannabis to help with symptoms and sone people start pregabalin or gabapentin about a month before last dose. I had a terrible withdrawal but a few people seem to manage without too much trauma.
Make sure your ferritin is above 100, preferably 250 as that can help as well.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.