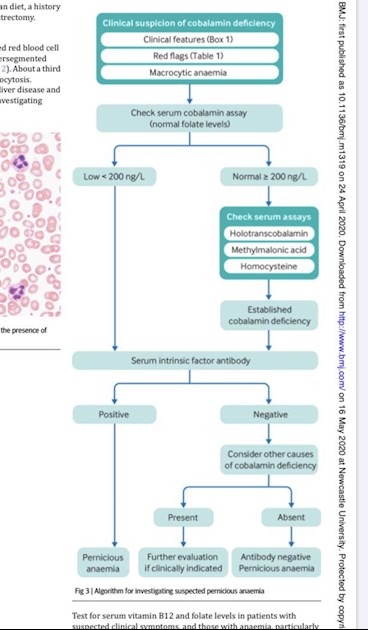
Also interesting that the recent bmj article defines a pathway for non-antibody PA for those with b12 levels lower than 200ng/l where no other cause is found.
Recent bmj article - flow chart - Pernicious Anaemi...
Recent bmj article - flow chart
Written by

Dexy123
To view profiles and participate in discussions please or .
Read more about...
9 Replies
•
Or those with a 'normal' serum B12 but abnormal 'active' B12, MMA, or hCys.
Yes, I get the impression that the NHS doesn’t usually routinely investigate using these tests - or maybe I’m wrong?
Here is one from a great hospital in the US, May Clinic
Gambit62Administrator
The diagram is drawn from the BCSH standard on diagnosis and treatment of cobalamin and folate disorders.
Ok great - thanks for letting me know as I wasn’t sure how it compared to previous charts. I just thought it might be helpful reference point to recent evidence for anyone who has had their injections stopped due to the pandemic and who has been diverted onto oral tablets. I know the chart raises several questions about the treatment decisions made by my gp!
CherylclaireForum Support
The trouble is that people seem to run out of steam with diagnosis by elimination.
It's the getting people to make a decision about what is wrong with you that is difficult. Comparatively easy to get consultants to tell you what you don't have, but that list can be endless. Some tests would not be useful once treatment has started and most consultants have too long a waiting list to risk going untreated for that length of time.
I started with a very good GP who found I had B12 deficiency (below 200 ng/L), low folate, ferritin and vitamin D- and got my MMA test done when I started getting worse on 3-monthly B12 injections after loading completed. She also eliminated any chance of renal problems being the cause.
She diagnosed functional B12 deficiency based on a raised MMA despite a serum B12 of then over measurable amount (above 2,000 ng/L) - and the laboratory confirmed this. Reloading started ( 2 injections a week) and I started to improve. My doctor's certificate read "severe B12 deficiency".
Then I went beyond primary care because reloading eventually stopped improving six months later. So began elimination tests by consultants - not SIBO, not Coeliac, etc etc. Decision that raised MMA is probably "my normal".... but no-one to tell me why four years on, I still have B12 deficiency symptoms that cannot be attributed to anything else.
I have been very lucky. Due largely to the persistence of my GP, everything that can be done, has been done. I've even had my DNA tested. This must have cost a fortune.
So I believe my GP was right, and I believe that the answer to functional B12 deficiency is frequent injections, and I believe that I am doing well now on one injection every third day, reduced after 2 years from every other day. Perhaps I will be able to reduce this further without deteriorating - but it's not possible yet. There are no real guidelines for this.
The only real research I have read is from Taylor and Talbot in 2009, where frequent injections suggested.
We don't seem to fit neatly into those boxes, do we ?
"Low B12, raised MMA, IFab negative" doesn't really cover it !
I have a very useful resource on all of this but am not able to mention it to current practitioners and that is a very good friend who was a GP. He is getting on now so is no longer in touch with the modern stuff. He has very little patience with the current crop.
He takes the view with B12 deficiencies that if it works don’t rock the boat. It doesn’t matter what the numbers are treat the symptoms and if an injection every day is needed then so be it. He used to keep the 2 appointment slots in the morning before surgery and after surgery in the evening for things like that and emergencies. As he often reminds when he started out there were a couple of dozen bottles of ‘medicines’ on the shelf in the little dispensary off the surgery and only a couple of them did any real good. If you had something which worked then use it.
I have discussed all of my problems with him over the past twenty years and it has been great to have a friend in the enemy’s camp. (He gets his many computer problems sorted by me in return.) It does mean we can both go to the official experts with fully loaded weapons in out armouries.
Not what you're looking for?
You may also like...
Recent bmj article - patient preferences
Interesting that the recent bmj article on PA indicates that oral versus injection of b12 should be...
Rapid responses to recent BMJ article
Thanks to @[1170824]and @[1070392]for mentioning this article.
I wondered if people had seen the...
New Response on BMJ Article!
Linky
http://www.bmj.com/content/349/bmj.g5226/rapid-responses
The BMJ - Article on Vitamin B12
Hi Guys
I thought this may be of interest:
https://www.bmj.com/content/383/bmj-2022-071725
If I...
BMJ Vitamin B12 Deficiency by Hunt
Hello
I haven't got the direct link and don't want to upset the powers that be in the BMJ by...