I was reading Simon’s latest article about the PD drug development pipeline, which is a good read anyway - scienceofparkinsons.com/202... - and watched this video from Dr Kelly Mills of Johns Hopkins University about disease-modifying vs symptomatic therapy - youtu.be/3y-1jeJcp-4 .
There are some interesting conclusions:
- As the disease progresses and we need to take more C/L, it’s not because we’re addicted, it’s because the brain needs more dopamine.
- Earlier use of levodopa does NOT mean earlier dyskinesia and wearing off.
- Some of the risk depends on how long you have had PD, NOT how long you have taken levodopa. (his emphases).
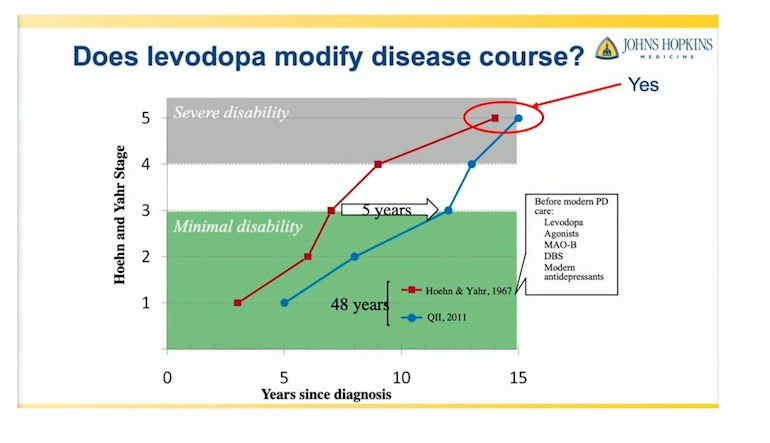
- Taking levodopa may slow down disease progression. He shows the graph above comparing progression through the various Hoehn & Yahr stages from the pre-levodopa era compared to the current treatments. For example, the data suggest it takes 5 years longer to reach H&Y stage 3 when taking levodopa than when not. Of course, there are other drug classes but levodopa is used overwhelmingly more than others.
- So not only do people progress more slowly through the Hoehn & Yahr stages of disability but they also get the benefit of symptom relief and improved quality of life.
- Exercise, exercise, exercise.
Then there is this surprising recent paper - onlinelibrary.wiley.com/doi... showing that levodopa inhibits alpha-synuclein accumulation in a non-human primate model of PD in all the brain areas tested except, unfortunately, the substantia nigra. It’s doing something unexpected, though. I couldn’t get to the full paper as it’s behind one of those infernal paywalls.
I think this is yet more evidence that PwPs should start taking levodopa (and IMO one containing a known dopa decarboxylase inhibitor as in Sinemet or Madopar) as soon as they need it, and AVOID LEVODOPA-PHOBIA!!
Written by
Cagey84
To view profiles and participate in discussions please or .
I vote Yes for having it become a "STICKY" , that is that it is one of a group of
"THE Best Basic Descriptions of WHAT PD IS and HOW It progresses over time"..... IMHO
A "STICKY" , on another forum on Solar power , was permanently placed at the top of each all the various discussion groups, which the moderator would have to develop as I have yet to find such a Key or Index to this great forum.
I would be one of a few outliers on his graph at the end as I was diagnosed with PD almost 7 years ago and have had symptoms for 30 years + and am still in stage 1 with only slight expression of 1 stage 2 symptom.
Congratulations, Sapeye2020, for doing so well after 30 years! Can we assume then that you started C/L early on in your progression? Might you be willing to share any other things you have done over those 30 years that you attribute to such admirable slow progression?
I was in a serious car accident so a lot of the symptoms were attributed to broken ribs etc. I swam 3 times a week, played water pool, a contact sport, I had an outdoor forestry job for20 years so lots of walking , etc. Constant massage treatments, lots of homemade red wine and a wife that keeps me moving since I retired, cut a large lawn with a push gas mower, cut wood for the cook stove /heater at the cabin.
JUST KEEP MOVING AS FAST AS YOU CAN, WALK THE DOG TWICE A DAY.
I think it’s entirely normal for newly diagnosed pwp to think they will be different , they will follow their own unique way through. At first it’s usual to look for ways to fight the disease without medication, explore alternative therapies that would uniquely change the course of the disease. Over time it becomes apparent that levodopa works pretty well and there’s little point avoiding it. Most are then grateful to have it. This is a journey most folk take.
The doctor in the video does not claim levodopa may slow that the disease progression. He speculates that levodopa therapy allows the person a healthier lifestyle and more exercise which is what slows the progression. Nor does Simon Stott claim levodopa slows the progression. The current (today) position of the Michael J Fox Foundation and the National Parkinson's Foundation is that levodopa does not slow the progression.
I assume everyone understands that MPTP mouse model is not a mouse with Parkinson's. As one might expect, injecting hydrogen peroxide in the brain of a mouse causes movement disorders such as loss of balance, dexterity, motor control. Injecting another synthesized molecules into the mouse which ameliorates those conditions may allow the researchers another grant if they get publicity, but in the real world, that is, the world in which we live, it is not really a breakthrough.
As to the rest of the evidence as to why we should not suffer levodopa phobia, I don't much care what happens in vivo, in vitro or in petri dishes because it will have no effect on me in my lifetime.
This is another regurgitation of the sub-Saharan African study which draws its conclusions vis-à-vis dyskinesia. The conclusions of such studies do not apply to everyone equally. They apply in varying degrees to various segments. If you are not taking levodopa, you cannot get levodopa induce dyskinesia. A PWP can get dyskinesia from any dose of levodopa over any duration such as a few months or weeks. There are people on this forum who have gotten dyskinesia from their very 1st, minimum dose of levodopa - as in 15 minutes.
Levodopa does not benefit everybody and for some it's side effects are worse than their symptoms.
The vast majority of PWP take PD pharmaceuticals, consider them essential, are well served by them and I totally and completely support that decision. I, however, have decided to delay the initiation of levodopa therapy for what I feel are good reasons and someday I'll bloviate precisely on those in another thread.
Hi Marc, thanks for the reply. I’d read previously about how dismal the lives of PwP were before the advent of levodopa, when life expectancy was lower (pubmed.ncbi.nlm.nih.gov/185... ), but I hadn’t seen the curve that Dr Mills showed. Of course, a lot of other things have improved since then as well, including recommendations on exercise so it’s probably not 100% down to levodopa. This is consistent with the graph shown by Dr Mills.
The reference point for comparison is key to this. Pre-1970 management of PD compared to today is vastly different and I would argue owes a lot to the advent of levodopa. Comparing 2020 management of PD with or without levodopa is highly unlikely to show a disease-modifying effect within the limits of the trial designs that are currently used. A prospective long term (say, 5 years+) delayed start study to compare levodopa and placebo hasn’t been done. There again, no disease-modifying trials have yet worked, although the longest study time that I’m aware of was the 3 year study time for isradipine. There could also be ethical issues doing a study that denies dopaminergic symptom relief to a placebo group.
I agree with your comment about rat and mouse models with MPTP/rotenone/etc. However, the paper I’d seen used a monkey model to look at alpha-synuclein aggregation in different brain regions – not symptoms. There is a clear biological effect that is intriguing but this is not proof of disease modification – there’s enough debate about alpha-synuclein as it is. It does suggest that levodopa may do more than just relieve symptoms.
Then we come to the long-duration effect of levodopa which can be measured some time after washout. This paper - pubmed.ncbi.nlm.nih.gov/328... - also in sub-saharan PD patients, assesses this property in a small group of patients. This group tried to quantify the long-duration response - pubmed.ncbi.nlm.nih.gov/302... .
Then we have the side effects of motor fluctuations, bad off time and dyskinesia. It seems clear to me, not just from Dr Mills’ presentation or the sub-saharan study but from almost everything I’ve read and heard, that these side effects are due more to the level of neurodegeneration than the dose of levodopa. Despite that, it makes sense to use as little as is needed to give the required symptom relief.
I agree with you that we’re all different, some of us on levodopa will get dyskinesia early; others not at all. I respect your decision to delay levodopa; it’s your disease, it’s your choice. The same applies to anybody who can’t tolerate it. The main reason I wanted to write the post was the regular messages to newly diagnosed PwP not to take medication, or to be scared of it. They shouldn’t be wary of the medication; the disease is tough enough to deal with and medication plus exercise is the best prescription.
I agree with much of what you said. Again, the vast majority of PWP take PD pharmaceuticals, consider them essential, and are very well served by them. The significance of levodopa therapy cannot be overstated. I am completely and totally supportive of that decision.
I do believe, however, before any person takes any pharmaceutical, they should have a thorough understanding of what they're getting into.
I do not believe that 90% of the people who are prescribed levodopa in the doctor visit where they are told they have Parkinson's, have it explained to them that the drug does not affect the underlying disease.
I don't believe the jury can be brought in on the cause of side effects. Personally, I believe the side effects we're talking about are due to the drug.
I've read each of the links you provided and do not see that they allow for the explanation that the pharmaceuticals provide a better opportunity for a more robust lifestyle. I do believe the jury has been brought in on whether not Parkinson's pharmaceuticals have a direct effect on the progression and I am satisfied that none do.
I have yet to get my arms around the conclusion of the sub-Saharan study that because it is the dose, not the duration, there is no reason to delay the therapy. I don't see how the conclusion follows from the data. I think a more precise conclusion would be, "Therefore, one should try to avoid escalating their dose as much as possible."
Also, I am not convinced it is legitimate to compare Ghanaians to Italians. I can't imagine they have much in common except 2 eyes 2 ears and a nose.
Anyway, I do not believe the decision as to when the start levodopa therapy should be based exclusively on when it is likely to induce dyskinesia.
Bottom line, I would like to see newly diagnosed people be as well-informed as possible and unless one reads or hears both the pros and cons, one is not well-informed.
I don't reject the study outright. I just don't understand why everybody would base their therapy decisions on this 1 study.
This post and your later ones are a very good analysis of the sources cited by Cagey84 in light of what is reality and their obvious flaws. Your best posts in ages. Unfortunately, unacceptable to many regardless of the validity of your perspective.
Not to put too fine a point on it, but , when one considers 1) how much influence gene expression and our microbiota have on Parkinson’s and 2) how much influence diet has on gene expression and our microbiome and 3) how much influence diet has on pharmaceutical absorption and half-life, they are hardly identical cohorts. (I don't see how is possible to have adjusted for this difference.)
“The Ghanaian diet largely relies on starchy roots (cassava, yams), fruit (plantain) and cereals (maize, rice). Starchy roots and cereals still supply almost three quarters of the dietary energy and diversity of the diet remains low.”
Whereas the Italians eat a Mediterranean diet. I eat a Mediterranea-ish diet because I believe it’s best for Parkinson’s. Lots of fresh fruits, fresh vegetables, fresh fish, lots of diversity. Pretty much the opposite of what the Ghanaians eat.
Well, to put a very broad point on it, diet is just one aspect of "idiopathic" PD causation. Certainly valid, but not the single independent variable. We have multiple "confounding" variables....head trauma (CTE, TBI), air pollution, water pollution, food pollution, land pollution, pesticides, herbicides, detergents, solvents, heavy metals, chronic stress, family genetics, vascular CVD, gender, old age, certain drugs like meth, etc.
the problem is that levodopa is a poison (almost can't be found in the nature) and doesn't work for a long time . Why researcher don't look for other better dopamine precursors' ?Haven't they be found?
Hi b-bar, I think it's wrong to describe levodopa as a poison. It's a natural compound that you could find in your dopaminergic neurons as it's on the synthetic pathway to dopamine. It's also found in some plants such as mucuna and fava beans.
I was interested in this question for a while, after I saw a presentation at the Movement Disorders Society conference on MSA that compared life expectancy after diagnosis between MSA, LBD, and PD before and after the advent of dopamine replacement therapy. The life expectancy of PD patients before the advent of dopamine replacement therapy was not much better than that of people with MSA. So it seemed a fair question to me that it if this is indeed the case that it increases life expectancy ,then should it not be considered disease modifying?
I had been thinking I would post on it if I had time to follow up, read up on it and document sources since as you point out there appears to be some 'levodopa phobia'. I kept feeling bad about not trying harder to get it done ... but you did it already! Thank you!
I believe the explanation would be people live longer because levodopa therapy affords a higher quality of life and the opportunity for more vigorous exercise which is what extends the life.
This could be flipped around to say a person who does not take levodopa lives longer, but if we examined why and found the same pattern, a robust lifestyle regimen, that would explain it, so we cannot conclude that people devoid of pharmaceuticals live longer.
The fact is, Parkinson's pharmaceuticals have no direct bearing on our health and I hope we fully appreciate the implications of that which are; if a PWP is treating their PD with pharmaceuticals only, that is, to the exclusion of everything else, they have no chance of improving their situation/health.
I agree that lifestyle interventions, particularly exercise, are really valuable.
Maybe dopamine replacement therapy increases life expectancy (if it is true, I would still like to see the data myself, but the information on it slowing progression seems to suggest it is) by increasing ability to do exercise - it seems likely, but it is also possible there are other mechanisms at work. Dopamine does a lot of stuff; it appears to play a role in the regulation of autophagy, for example.
I don’t know about life expectancy but Levodopa must be responsible for improving the mental health of pwp. Being mobile and feeling normal for a time allows some normal activity, social engagement, exercise etc. Without, life would be more limited and challenging. There is a balance though and in my view levodopa should be used sparingly and increased only when really necessary. I accept some slowness and off times and don’t expect to be good all the time. But that’s just me .
I really wish I knew exactly which presentation it was. It says the same thing on the wikipedia page on dopamine replacement, but no reference is given. It was the MDS virtual conference this past September.
Oh well, it doesn't matter as I no longer have access to the videos since I'm not an MDS member. That's what I get for not taking notes!
I think we're missing the significance of the word 'facilitates. ' Levodopa facilitates a longer life, but is not directly responsible.
It would be like saying I use my car to drive to the grocery store (the result of which is I eat and therefore I live ) and therefore riding in the car makes me live longer.
In other words if a person took levodopa but did not take advantage of it providing the opportunity for a better lifestyle (psychological included) that person would not live longer.
Otherwise, we have to see the data and to date I've seen none.
PS> This issue - whether not PD pharmaceuticals directly slow the progression is probably the single most important issue for each of us to figure out, that is, base our therapy decisions on. I fear that people who believe their pharmaceuticals are slowing the progression affords them the rationalization to be less disciplined and work less at their own health.
I agree. The most prudent course of action would be to do everything possible to slow progression, based on risk/benefit ratio. Exercise has an excellent risk/benefit ratio, of course.
However, it seems like some people think that dopamine replacement therapy will cause more harm than good and it looks like this is not the case & may in fact be the opposite. It is surprising there is not more definitive information on this topic - perhaps with fitness trackers a large epidemiological study could be carried out to effectively tease out the effects of activity vs. drug effects - I don't know if that is possible. Perhaps it doesn't matter if people are told from the get-go they need to exercise as much as possible.
I believe there is already a sufficient number of studies on the effects of physical exercise to conclude exercise does slow progression.
Well, certainly with most people it does not cause more harm than good, but we have to remain mindful that in some people it does. Several people on this forum have said the side effects are worse than the symptoms. Some people report that it worsens their symptoms. Some people report dyskinesia within a few weeks, so, in other words it is not always clear-cut, "Take this drug and you will be fine" isn't always true.
And I believe people should keep in mind that their doctor has no possible way of knowing what affect levodopa will have on them. The only way to know that is to take it.
I just think we should be extremely cautious and not willy-nilly pop exotic drugs in our mouth.
I hope in future they will be able to better predict peoples' responses to drugs using pharmacogenomics. After my daughter's experience with neuroleptic malignant syndrome from Reglan I looked into it and it seems they don't uses it in clinical practice yet - even though there is already a review article on the pharmacogenomics of Reglan. She had some TD for a few days after; her blink rate is still elevated. Your point on some people getting dyskinesia after the first dose is well-taken.
She was in an eating disorders unit since she had lost a lot of weight due to intractable vomiting and was initially misdiagnosed with avoidant restrictive food intake disorder (ARFID) - a really rare eating disorder. It turned out she has Celiac and Oral Allergy Syndrome. During the NMS incident, they kept insisting she was having a panic attack and the pediatrician on call wanted her to take another dose of Reglan. Of course we refused since it was obvious to us (mom and dad) she was
having some sort of adverse drug reaction. She had had tremor all day
after her first dose of Reglan the previous night. If she had taken
another dose of Reglan, she probably would have died. The resident
assigned to her case figured it out the next day. I had thought it might
be serotonin syndrome; it occurred around 15 min. after her evening
dose of Zofran (Zofran had previously not caused any problems). She was
also on a very high dose of proton pump inhibitor (Protonix), which can alter drug kinetics and inhibit V-ATPase. There were some differences
with what I've seen listed for NMS - she did not get a high fever and
she seemed remarkably well-composed and cognizant despite having
problems breathing (at one point her lips turned blue) and not receiving
she still has nightmares; I do too, weirdly enough one is about her being on a ventilator and me watching from far away - this was before the pandemic.
I'm so pissed at myself for letting them give her the Protonix since I figured it would be bad as I already knew what it could do to V-ATPase. I'm upset I ever took her to the hospital to begin with - I was scared about possible heart problems. Her transglutaminase antibody level is still high, despite being GF. She appears to have essential tremor now (postural tremor), mostly just when tired. She's on an SSRI, which can cause that.
I think most people, myself included, are reticent about taking drugs unless we absolutely have to.
Prescription drugs along with stroke are the 4th leading cause of death killing 128,000 people a year in the US in 200,000 per year in Europe. Not an encouraging statistic.
an ethics blog from Harvard
"New Prescription Drugs: A Major Health Risk With Few Offsetting Advantages"
"Few know that systematic reviews of hospital charts found that even properly prescribed drugs (aside from misprescribing, overdosing, or self-prescribing) cause about 1.9 million hospitalizations a year. Another 840,000 hospitalized patients are given drugs that cause serious adverse reactions for a total of 2.74 million serious adverse drug reactions. About 128,000 people die from drugs prescribed to them. This makes prescription drugs a major health risk, ranking 4th with stroke as a leading cause of death. The European Commission estimates that adverse reactions from prescription drugs cause 200,000 deaths; so together, about 328,000 patients in the U.S. and Europe die from prescription drugs each year. The FDA does not acknowledge these facts and instead gathers a small fraction of the cases."
Having thought about it overnight, here's a better way to explain my decision.
Every person diagnosed should expect it inevitable that at some point they will need levodopa and that over time the dose will continuously be increased until at some point they will experience levodopa induced dyskinesia (LID.) And, so, the goal becomes to delay that inevitability for as long as possible and the only way to do that is to combine lifestyle, diet, exercise, and supplements with the slowest possible escalation of dose. And, if one starts levodopa at the time of diagnosis, they will be taking a higher dose 8 years later than if they start levodopa 8 years later.
Mark, I do not believe that your assumption of the speed of disease progression in both use of Levodopa and no use is the same. My reason is that the speed is dependent on so many things, ie exercise: type, amount , intensity, etc is a large factor in your stasis or degradation without considering the amount of Dopamine available in your body, let alone using C/L.
I am (also) trying to rationalize my present state of body vis a vis Quality of life/Covid 19 presence/ and exercise where going into the pool heightens my chance of exposure to Covid19.
I say this as with the onset of winter, ice, falls, physical safety, etc has caused my physical state to degrade.
SWMBO wants to go to Canadian Tire for a new mop.. back in a while.
Can I assume SWMBO is the spouse? Yeah, it's a dilemma. I haven't been to the gym in 2 months and am paying a price for it (weaker.) The gyms reopened here Saturday and now I'm going again -- gripped in fear. I think the young people who go to gyms are already one notch above the normal level of self absorption of young people - so, of course, not all of them can be bothered to wear a mask. I carp at them, though. Being an old coot, I get away with that.
We are on the same page. You reiterated my point. Because levodopa reduces symptoms and allows for much less difficult body movement, people on levodopa are likely more highly motivated to be disciplined about diet and better able to exercise, so they progress slower. A person who takes levodopa and does absolutely nothing else will almost certainly progress faster than a person who has a robust lifestyle (sleep hygiene, stress management, social engagement, adequate nutrition/supplements, weight, flexibility, and aerobic exercises, etc.)
Hi Marc - the following paragraph in this good review - link.springer.com/article/1... - captures the issue ideally IMO:
"Based on these observations, most experts introduce levodopa when the patient requires it for symptomatic and functional benefit as evidence is lacking to indicate that it should be started immediately upon diagnosis (irrespective of any functional impairment) or that it should be delayed as long as possible. However, there is general consensus, with good supportive evidence, that levodopa doses above those required for adequate control of symptoms should be avoided as higher doses may unnecessarily increase the risk for motor fluctuations and dyskinesia."
However, I'm not sure about your last sentence. If that was true, it implies that levodopa causes neurodegeneration, which I don't think is correct.
I like the paragraph in quotes. My sentiments exactly.
Are you referring to this sentence, "And, if one starts levodopa at the time of diagnosis, they will be taking a higher dose 8 years later than if they start levodopa 8 years later."?
By that I was trying to say that if a person starts levodopa that the time of diagnosis, 8 years later, they're likely to be it 6 or 8 pills/day, (or 10 - 20) whereas if a person is just beginning levodopa therapy on their 8th year, they will likely start at a much lower dose.
I am working on a W10 machine that did a BIG update last night and it took me to ALL of Elliot's postings . were you pointing to a specific post? Firefox took me to the exact posting wanted, before the update and I now can not get it to be my chosen Browser... and now to get at the smilies you have to have a name???
Hi Marc, yes, it was that sentence. My point is that if, after 8 years without levodopa, you would start on a lower dose than an 8 year levodopa veteran, then that suggests levodopa has contributed to greater nerve loss. I don’t think this is the case. Surely, if we assume that levodopa does not affect disease course one way or another, the level of nerve loss will be the same and require the same level of symptom relief?
I do not mean a person who is taking levodopa for 8 years would progress more than a person who is not.
Essentially, I am saying simply that whenever a person starts a drug, they start the minimum dose.
I am trying to say that whenever a person starts levodopa therapy, they start at the lowest, minimum dose whether that's one year after diagnosis, 5 years after or 8 years after and if that's not enough, they work their way up. I doubt a person just starting levodopa therapy no matter when that is, starts at more than the minimum dose or not much more than the minimum dose.
I believe the standard starting dose of levodopa is 3, 25/100 pills per day. I believe after 8 years of typical progression the average PWP is probably taking somewhere between 6 and 20 pills per day. I did not take levodopa the 1st 8 years after diagnosis. I started tinkering around with it a couple years ago. I started at 3, 25/100 pills a day.
While having this discussion previously, others have said that a person who is 1st starting levodopa therapy after waiting 8 years, would start at the same dose they would be at had they start at the time of diagnosis.
The main reason this does not happen is because there is no way to know what dose you would otherwise be at.
After waiting 8 years, I cannot imagine anyone agreeing with their doctor to start 6 to 10 pills a day, or whatever is the average dose after 8 years.
I have seen this theme debated, discussed many times here. This is the first that I remember that was done civilly , without personal insults and irrational behavior. We must continue , this is the most important question here. Wikipedia has stated a conclusion without any reference to a scientific study or any body of data or agreement.
I like Wikipedia and give them $20 a year, but we have to be careful with their medical stuff. Unless there are citations, I consider it of little or no value.
I have discussed PD with many old Parkies who are also playing the end game and notice a similarity to how their PD has progressed. Most have said that their expieriance is similar to mine in that.
The progression was very slow at the beginning for several years, but there came a time when it is described as "having a bad day" , the medication did not work as well and symptums increased and everything was wrong. I shrugged it off and said it would be better tomorrow . It was not. After several of these bad days I understood that that it was not a one day event but instead the new normal. Now the frequency of these days has increased and the severity of each change seems to be increasing. It has been suggested that at the time of diagnoses, when PD is just starting to show, that we may already have lost 70% of our cabability to produce the nesesary Chemicals ( which are more than just Dopamines ) It then might be suggested that the body does a great job of making the best of a very small amount but it then eventually crashes. I understand that at that point we could take all the Levadopa we wanted but the brain could not do anything with it.
So , proof seems to exist that exercise delays all that but there is not such proof of an increase in longevity for taking the meds nor for not taking the meds.
Maybe to me , the quality of my life is more important than the length,then I know which road to take.
I have seen many studies showing that prescribed PD medication does not shorten the overall life span, it is not "poison" and that trying to avoid medication if taken to the limits , too long ,creates stress and depresion and eventually you have a really bad day . Parkinsons expieianced at 40 years old or 50 or 60 does not much resemble PD at 72 nor 80.
The pictures painted of this deseace seem purposly blurry and I believe that is a result of younger Parkys just not accepting what PD is and they do not want to hear it.
I try to make them understand . I knew a man in his 90's that lived a happy (although quiet ) life with severe PD. Short skinny wirey man with white hair and a cane. He walked every day in the early 1970's with very little help from medication until one day he stayed in bed .
I appreciate your being more interested in the quality of the life you have left rather than how long you're going to live.
We have 2 options. Work as hard as we can to stay as healthy as we can for as long as we can, then work twice as hard to keep a good attitude and live in the present. I don't want to talk about the alternative.
We have many time saving appliances , faster computers with brilliant time saving APPs, and I wonder what we are saving it for and when we will get to use it. Sometimes it seems like people think we get a second chance , a redo, because they work so hard and retire late boasting about the increased pension that late retirement gave them , and then they die.
Mortality is discussed very seldom in a western society , its not warm and fuzzy and that may have consequence in our planning. Reality can be a cold thing.
I think some decisions to delay taking meds may be like that, the best years somewhat spoiled to make the last years maybe better.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.