It looks like a careful study and meets my quality test req't that I can follow it well enough.
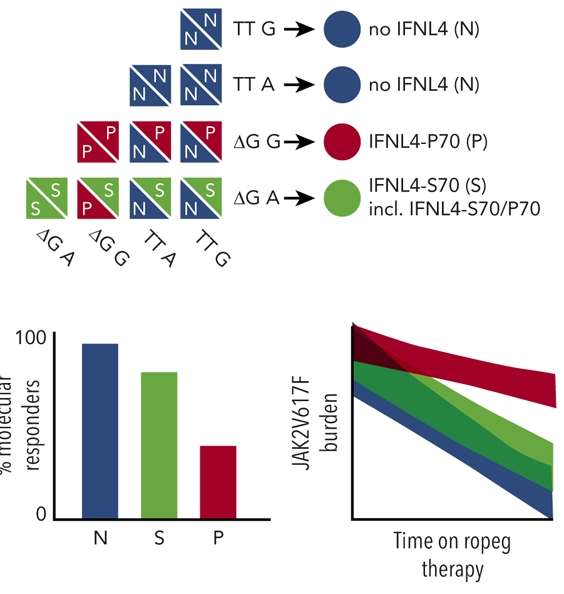
They found a gene that had a singif effect on MR (molecular response to reduce Jak2) inPV. It is IFNL4. If it has a certain "diplotype" status.
This is a germline gene, I believe meaning it's in every cell from birth. If you have the red P70 version in this chart, you get the red line that had much less MR. I think they found that a well working IFN4 is not desirable, and in fact having none at all was good.
In sum, if we could choose (we can't) : We want no IFN4 at all as a first choice or the broken one IFNL4-S70(green line) -2nd choice. But we don't want IFNL4-P70.
Maybe this sort of thing lends to gene therapy, ie deliberately change or get rid of it before starting IFN. For sure it's not that simple since other risks are unknown, but it comes to mind.
This gene had no effect on HR.
-I didn't have this one in my NGS panel, but mine was only 54 genes. Is there any member who did?
Written by
EPguy
To view profiles and participate in discussions please or .
I had gene sequencing done in June 2022 by my MPN specialist at the University of Pennsylvania. IFN (nor any variation) was not among the 116 genes sequenced.
A germline mutation is defined as « any alteration in the genetic sequence of genes of the germinal cells ». So it does not affect « every cell in the person » but only the germinal cells (found in gonads)…and not the somatic cells.
So, can I make the leap that our driver mutations and others like ASXL1 and SRSF2 only affect the hematopoietic stem cells in our bone marrow or in bone marrow plus extramedullary hematopoiesis sites? Or do some of these mutations affect cells everywhere and possibly cause other cancers?
And are karyotype anomalies such as del(20q) in all of our cells?
Please see my response below to EPguy a few minutes ago. That might be a better place to respond with any corrections or explanations.
I had some clue on germline only because my BMB found one that was " seen in all the cells analyzed" and they called it a "germline change" rather than "an acquired abnormality". (as our Jak2 etc is) The term "change" suggests it happened after conception. As Manouche notes here, maybe there's two types of Germlines?
Apparently it shows that you have some changes (inherited not acquired) in the bone marrow stem cells/germline(?). It would be interesting to ask your haem.
The mutation was reported as- not known to be hematologiclly relevant, so the Hem field probably won't have much to say. So far my endless curiosity has not taken me to look further into this one, searching for these breakpoints has not brought up any relevant hits.
"ABNORMAL male karyotype with an apparently balanced translocation involving chromosomes 4 and 6 with breakpoints at bands 4p14 and 6q13 in all 20 metaphases analyzed...This particular translocation has NOT been reported in association with a hematological disorder..."
If it hasn't made trouble yet by age 63 I guess it's probably not going to.
I did see that one. But I can't find the 4p portion there that 6q13 needs to exchange with. I know little of these, but I think tiny details make a big effect. ie v617f Jak2 is so small a change.
If it is reproductive, that's my last worry so no worries, but it seems likely something else.
Our no-good Jak2s reproduce all too well, that's why it's common to see VAF (how many jak2s are mutated) go up over time, they clone faster than the good ones. This is what cancer does, and why MPN is now called cancer.
IFN can help the immune system go after these bad clones faster than the good ones, so our VAF can decline with IFN therapy.
Again, to clarify, the JAK2-mutated stem cell proliferate by cloning uncontrollably , normal stem cells do not reproduce themselves- they only make blood products.So:
" they clone faster than the good ones."
is technically incorrect- the clones out produce and out-survive normal stem cells, that's why ,once they burn themselves out into myelofibrosis, patients become anemic- there are [is?] a dearth of normal stem cells left to make blood.
There seems to be some sort of reproduction, replacement, or even expansion process of normal HSC cells, at least in mice, and there is a division process that should inherently create at least temporary duplicates:
"We find that most HSC divisions in adult mice are symmetric self-renewing, replacing HSCs lost by direct differentiation and death, and slowly expanding the HSC population"
This report seems to cover these very issues in detail, but I need to get some work done.
--
This is consistent with what I think I've read of IFN, it enables the immune system to preferentially target the clones, (I now know where to use this word) but does not prevent all immune targeting of wild type. If so this would require the mouse process above to maintain a functional wild type HSC population (this is re ET, PV)
--
Another report discusses that HSC usually do not reproduce, but can do so when needed:
"Hematopoietic stem cells (HSCs) are in an inactive quiescent state for most of their life." "To replenish the blood system in homeostasis and after injury, they (HSC) activate and divide."
This report even uses the loaded word "proliferate" re normal cells... "(HCS daughter cells) to activate further to proliferate and differentiate and replenish lost blood cells"
I'm getting a handle on this. As I get it, we might get a mutation, but it is not able to make more copies of itself (no clones). But sometimes a mutant cell mutates just right to be able to start making copies, then we get lots of clones (high Jak2 % for example)
Sort of like some Covid variants don't make trouble while some take over the world.
I deleted the post below here with confusing clone info.
That's my understanding. Same as a Covid virus that's a new variant in just one or a few people but doesn't spread to others. But we don't hear much about the ones (virus or MPN mutation) that don't spread since they stay quiet and harmless.
It's been called an example of "survival of the fittest", works for both good and bad things.
If we have for example 20% VAF Jak2, would that mean that 80% of the Jak2s make normal clones ie the clones are 80/20 normal to mutated? I know not much on these details.
Hi EPguy,Clonal hematopoiesis is always a pathological process. Normal non mutated Jak2 cells don’t make clones but follow the normal hematopoietic differenciation/growth process.
<< it is thought that this subpopulation is "clonally" derived from a single founding cell and is therefore made of genetic "clones" of the founder, (where the founder has a) unique mutation in the cell's DNA.>>
Normal duplication of HSC is "Self Renewal without differentiation". I think a "clone" is specialized type of "Self Renewal", where a mutated cell also self renews without differentiation and these copies are all mutated.
--
According to this idea:
Normal Cell-> Copy of Normal Cell- is called Self Renewal without differentiation.
Normal Cell-> copy error->Mutated Cell -> Copy of Mutated Cell- is called Clone (A specialized Self Renewal)
And in cancer the clones usually copy faster than the normal cells.
Does this seem right?
This reference has one contradicting idea that a clone is any HSC, normal or mutated, that reproduces faster than expected.
I just downloaded most of that list of article for [an attempt at] future reading- but I suspect that a lot of it will be too esoteric even for me [as a medical guy and very involved MPN patient] to understand all of it.
I can't get too much from it. It seems MPNs derive from a single type of mutant cell, while some other conditions derive from multiple mutated cell types. This does match what I've seen, that MPNs are sometimes studied for general knowledge because having just a single mutation source makes some studies easier.
A normal hematopoietic cell doesn’t grow through clonal expansion. Unlike normal cells, a pathological clonal process implies 3 things : 1) molecular mutation, 2) clonal duplication, and 3) cellular immortality.
My understanding thus far. If my Jak 2 percentage was (for argument sake) 23%. That would mean 77% of my cells are normal haematopoetic cells (haven’t been affected by the mutation...YET), and 23% are derived from the Jak 2 mutation which has created a pathological abnormal clonal process in that 23%.?
I think your description here is consistent with the simplified scheme above, modified here:
--
- Cell line 1: Normal Cell-> Copy of Normal Cell
This copy Self Renewed without differentiation.
- Cell line 2: Normal Cell-> defective differentiation ->Mutated Clone -> Copy of Clone
This copy, of the Clone, also Self Renewed without differentiation.
--
Cell line 1 is for example wild type Jak2. Cell line 2 is Jak2v617f.
From what I read, some clone lines die out or don't expand but the odds favor an advantage to the clone line vs the normal line. IFN can flip these odds by capping clone self renewal and making the clones mortal.
Further if we have a positive Jak2 v617f result, by definition we have a clone.
Does all this seem right?
--
In a related item that comes up, elderly have lots more clones than previously thought and increased odds of progression to cancer. The mutations are familiar:
<<Clonal hematopoiesis with somatic mutations was observed in 10% of persons older than 65 years of age but in only 1% of those younger than 50 years of age. Detectable clonal expansions most frequently involved somatic mutations in three genes (DNMT3A, ASXL1, and TET2) that have previously been implicated in hematologic cancers.>>
Further in this ref, it shows how complex all this is:
<<Somatic mutations may be either drivers, which contribute to clonal expansion, or passengers, which do not; either could indicate the presence of a clone>>
Curious whether the use of "driver" is the same as we are familiar, ie non-drivers would not have expansion advantage. Other searching suggests there is an entire category of passenger mutations that don't have expansion advantage. How that's relevant to MPN I don't know.
If you're ok with it I'd like to post a summary of this learning experience so members can better understand what "clone" is about. My one sentence conclusion is it's a distinct (usually bad) type of cell renewal/duplication.
Well, yes, except that normal stem cells don't clone themselves.
That's what makes JAK2-possessing cells cancerous by definition- the uncontrolled cloning- which can eventually proceed to the point of causing clones to be active in non-bone marrow locations [like the spleen and liver] "extra-medullary hemopoiesis" , which is technically metastasis.
"Normal non mutated Jak2 cells don’t make clones but follow the normal hematopoietic differentiation/growth process."
is somewhat inaccurate.
JAK2 clonal stem cells are always [by definition] aberrant cells, which replace normal [non-JAK2-gene-containing] erythropoietic stem cells, which are regulated in their production of downstream blood products by erythropoietin secretion from the kidneys.
Having the designation of JAK2 [or CALCR, or whatever genetic variant they possess] is what makes them aberrant.
JAK2 clones are not regulated or otherwise affected by erythropoietin, so they just keep uncontrollably [by usual means**] pumping out whatever blood products they are prone to, and they also reproduce themselves uncontrollably [proliferating] as identical clones without end [until they burn out- transforming to myelofibrosis], hence the term myeloproliferative neoplasm [MPN]
[Neoplasm= a new and abnormal growth of tissue in some part of the body, especially as a characteristic of cancer.]
**This is where Interferon or Jakafi, and other potentially "disease-modifying" drugs come into play to hopefully provide control [down-regulation] to achieve both CHR [complete hemopoietic response] and CMR [complete molecular response].
See EPguy's post below for more details.
[Sorry, I have to stop coming into these discussions in the middle, and just go to the end before commenting...]
I'm well over my head on this level of genetics. But always happy to try learning.
I think Karyotyping looks at our whole DNA set, checking for the basic features being where they belong. In my case two genes were switched, thus in the wrong place. Genes can also be missing or added. But our Jak2s are right where they should be, so Karyotypong won't find anything wrong there. But the Jak2s are defective internally (are variants, mutants or alleles). So a Karyotype will find Jak2 in its proper place while the allele study finds that some Jak2s are defective.
So among countless genes, Karyotyping can check they are there and correct ones. But the lab needs to decide which ones to check for allele, doing them all would not be reasonable. In our case Jak2, CALR, MPL all may be suspect so they look among these. NGS (our deeper sequencing) looks at other genes known to be suspect in MPN, but still not all of them since that is not (yet) practical.
My guess is clone is about Karyotyping, but as above the term seems redundant since all genes get cloned. So think it's shorthand for something. maybe a wrong gene in the wrong place. I hope members with deeper knowledge here can help.
If you read thru this thread, its a tiny taste of medical school. This stuff is incredibly complex. If your Haem can help I look fwd to any info.
Based on this discussion, and skilled info from Manouche, your "no clone detected" matches your triple negative status. No allele, mutants, clones were detected. Most MPNs therefore will have clones detected. (Jak2 CALR, MPL and non-drivers)
Did you get nextgen sequencing? This looks for 100+ other various alleles/ clones/mutants.
I am afraid to have the NGS test cause if a high risk mutation been found i will be very stressed. So you think that Jak 2,Calr etc could have been detected and reported on the karyotype test??
I understand on the NGS. So far I'm not aware of changes in treatments that would result from this info, only in prognosis. But if/when that changes, it could be worth having.
My best but simple understanding on Karyotype is as above, reproduced here. These are fine details but might explain it, assuming this is the right path:
-Karyotyping looks at our whole DNA set, checking for the basic features being where they belong. In my case two genes were switched, thus in the wrong place. Genes can also be missing or added. But our Jak2s are right where they should be, so Karyotyping won't find anything wrong there. But the Jak2s are defective internally (are variants, mutants or alleles). So a Karyotype will find Jak2 in its proper place while the allele study finds that some Jak2s are defective.
-They find our defective Jaks2 etc only because they know to look at these specific genes. For MPN they check only the ones that are at risk in blood diseases, ie Jak2 etc + NGS if we get that.
My interpretation of a comment by my MPN: Clone and Allele or Allele Burden are equivalent terms.
I just looked at "alllele" on Wikipedia.org. Very interesting and seems to confirm my MPN's statement.
Looking at "karyotype" is also very educational. It appears that an atypical karyotype must affect cells throughout our bodies, or rather the percentage that are atypical. My atypical karyotype was present in 11 of 20 cells examined, so I expect that roughly half of my cells still have normal chromosomes. Oops, there's another word to look up to fill in my knowledge gaps!
Wikipedia is well worth the $2.75 that they ask us to contribute from time to time!
* We are conditioned by movies etc to think of "clone" as an identical copy. But in genetics it seems to be precisely not that; it is a modified and improperly differentiated copy, I've had trouble making this mental switch. Clones are subject to survival of the fittest, the ones we care about are malevolent (another movie theme). A successful mod (think Omicron Ba.5) proliferates, but some mods dissipate.
--
The part on allele is somewhat familiar. A location (among many) on a gene has a mutation. The two- Homozy vs Heterozy has been in posts, where homozy tends to higher allele% (since it's double the alleles) but also responds better to IFN.
--
I also had abnormal karyotype, but in all cells so it was called germline (generally at birth).
This was my current best of ability thoughts as posted above, note the term Clone added per your comment here):
"I think Karyotyping looks at our whole DNA set, checking for the basic features being where they belong. In my case two genes were switched, thus in the wrong place. Genes can also be missing or added. But our Jak2s are right where they should be, so Karyotypong won't find anything wrong there. But the Jak2s are defective internally (are variants, clones, mutants or alleles). So a Karyotype will find Jak2 in its proper place while the allele study finds that some Jak2s are defective (clones)."
Re this: "But in genetics it seems to be precisely not that; it is a modified and improperly differentiated copy"
That isn't my understanding- what you are describing isn't a cloning process, it's genetic mutation- which in my case [and apparently a bunch of others 😇] caused 1 stem cell to develop a Jak2 v617f mutation- which then began the "clonal" cellular reproduction process that has replaced approximately 40% of my hemopoietic stem cells with Jak2 v617f-containing cells.
These may also be [because of their unregulated and uncontrolled replication] prone to further "non-driver" mutations, which can affect their response to treatment.
Much of this seems to be semantic, and it's maxing my skinny brain. But I'm still curious.
One confusion for me is when does the defective cell acquire the name "clone". Is it 1- the original mutated cell and all its progeny, or 2- only the progeny?
According to this ref, implication is #2, the clones are what expand, while the 1st cell is not a clone, rather a "mutant". If so then the movie term matches, all copies of the mutant are identical clones.
<<Cancers are formed by the expansion of harmful “mutational clones,” which are cell populations carrying the same DNA mutations.>>
By this "clone" is a special type of "Self Renewal without differentiation" of a defect that (usually) duplicates faster than the wild type cells to overly expand the total cell population. This is essentially what you and Manouche say here, in a form I can maybe get my head around.
I added the "usually" because I've found in reports that only the successful clones expand (the ba.5 analogy) We don't hear about the dead end mutations.
In contrast, exact duplication of wild types without excess growth of the population is normal and properly assigned the term "Self Renewal without differentiation".
In this simplified scheme, there would be three named types, Wild, Mutant, and Clone, occurring in that order.
I can't argue with you about the semantics of it [or really anything else], as my only point was really that any cells which contain and express a JAK2 mutation are by definition abnormal, and that they seem to have a propensity for cloning themselves 'til death do us part, if no intervention is made- either to stop them from doing so [e.g., Interferons of multiple flavors] or to stop their effects- [Aspirin, phlebotomy, Hydrea [HU], Jakafi, and perhaps soon a Hepcidin mimic].
...and that normal erythropoietic stem stem cells only produce blood progenitor cells [
BTW, Here is what Merriam-Webster has to say about clones:
"Definition of clone
1a: the aggregate of genetically identical cells or organisms asexually produced by or from a single progenitor cell or organism
b: an individual grown from a single somatic cell or cell nucleus and genetically identical to it
c: a group of replicas of all or part of a macromolecule and especially DNA
clones of identical recombinant DNA sequences
2: one that appears to be a copy of an original form : DUPLICATE
a clone of a personal computer."
So properly, if I understood that, the original cell is the progenitor, and the identical copies are the clones.
However, the article you linked to [the pay-wall of which I could not pass], seems to make the point [this is just taken from the summary on PubMed] that colonies of clonal origin are way more common than we ever thought, and may not always become cancers.
That was news to me. However, upon reflection, just because it's a clone doesn't mean it's a cancer, because the defining characteristic of cancer is a clone that reproduces without regard to external [or internal for that matter] controls that would normally limit its reproduction.
I have to sign off now, but hope to start a new post later today to detail my visit to the BIG cancer CTR west of my location and what occurred there [and afterwards] yesterday.
It seems that a hematopoietic clone is always a cancer. To make things more complicated, a clone or sub-clone can indeed die out. It doesn’t mean they are not cancerous.
« Natural selection continues to act on the cells in the context of their microenvironment. Clonal populations with favorable phenotypes will increase in number, while those with neutral or deleterious characteristics remain stable or die out altogether ».
My ever-present brain fog again prevents me from remembering where exactly I read it, but I do remember reading that the JAK2 + hemopoietic stem cells [HSC] have a survival advantage over wild-type [normal] HSC.
This isn't the original source I remembered reading, but it does support that conjecture:
This is excerpted from the linked article:
"These results demonstrate that JAK2 V617F E-SLAM HSCs are more clonogenic and give rise to more progeny expressing differentiation markers under conditions that normally maintain HSC numbers....
I also found something interesting from here: originalText
"... Interestingly, other studies have shown that in MPN patients with JAK2 V617F and TET2 mutations, the presence of the TET2 mutation in single cell-derived clones conferred an advantage towards clonal dominance, but not JAK2 V617F on its own (103,104). Kent et al. in 2013 studied highly purified JAK2 V617F HSCs from a JAK2 V617F mouse model with an ET phenotype, and observed that the mutation reduced HSC numbers, but that early progenitors exhibited increased proliferation and differentiation (105). This result suggests that while JAK2 V617F confers hyperproliferation to the malignant clone within the myeloid progenitor population, it may be insufficient to establish clonal dominance at the level of HSC, and therefore that additional mutations or other pathogenic mechanisms may be necessary for clonal dominance to occur within the HSC population. ..."
While searching for the article I remembered reading, I also found this one:
Which makes me even more determined to press for Besremi in opposition to my heme/onc MD's expressed preference for Jakafi because of this:
"Early data from JAK2 inhibitor clinical trials have called into question the capacity of these compounds to alter the natural history of JAK2V617F mediated MPN. " and further:
"We further demonstrate that the HSC compartment, the definitive target for curative therapy of JAK2V617F mediated MPN, is resistant to treatment with a JAK2 inhibitor."
That's without even considering the possible increased risk of skin [and other] cancers and infection it may also pose.
A big reason we hear so much about Jak2 v617f is that it works so well in its nefarious purpose. We don't hear about the duds we'd rather have. You've likely seen the recent report posted by Manouche that is on these points. I take this report as a further endorsement of IFN.
This report found TET2 acquired before Jak2 had min effect, but it did not look at later TET2 acquisition, this might be what the study you have here looked at.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")