A fine example of evolutionary principles applied to metastatic PCa with the development of a method (Mscore) for risk assessment based on key gene mutations. (U of Texas and Chinese U collaboration.)
* * *
Abstract
Background Metastasis is the primary cause of prostate cancer-related deaths. However, the underlying molecular mechanisms and evolutionary patterns remain largely uncharacterized.
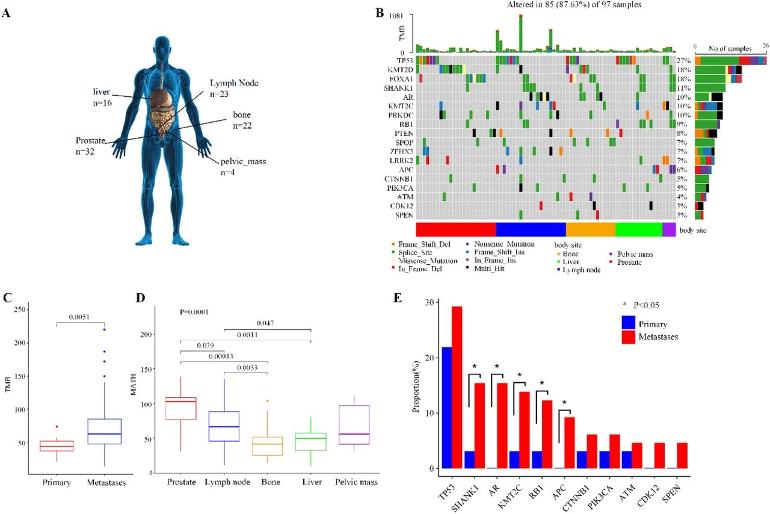
Methods We evaluate the heterogeneity and genomic evolution of prostate cancer with multi-organ metastases. The samples include 32 primary samples, 23 lymph node metastases, 22 bone metastases, 16 liver metastases, and four pelvic mess metastases. They are analyzed to identify the mutated genes enriched in metastatic samples, selected by metastases, and leading to different long-distance migrations. These metastasis-related alterations constitute a Mscore for evaluating the metastatic risk of primary prostate tumors.
Results Our analysis discovers 21 metastasis-related mutated genes in total. Of them, 14 genes are finally selected for metastatic risk prognosis, including the mutations of AR and KMT2C with high prediction ability. A Mscore established with these 14 characteristics by the xgboost model displays its ability to classify primary tumors and metastases. This score can further divide primary prostate tumors from the TCGA cohort into two groups. The two subsets present significantly differential survival risks. This score can also identify metastasis-featured primary tumors for breast cancer, bladder cancer, liver cancer, and uterine corpus endometrial carcinoma.
Conclusion Our research proposes 14 molecular features potentially driving prostate cancer metastasis. The Mscore established on them can estimate the metastatic risk of primary tumors.
* * *
Of special note is the following from the Results Section of the paper:
* * *
3 Results
3.1 The heterogeneity between primary and metastatic prostate tumors
Our pipeline identified 248 somatic single nucleotide variants (SNVs) and 163 somatic copy number variants (CNVs) across the tumors of 72 prostate cancer patients. Of the genes with somatic SNVs, the most frequently mutated ones were TP53 (27%), KMT2D (18%), FOXA1 (19%), SHANK1 (11%), AR (10%), and KMT2C (10%) (Figure 1B). Of the somatic CNVs in Figure S2, the most frequent CNVs included losses at 17q21.31, 16q22.1, and 6q15 regions and gains at 8q24.3 and 12q13.2 regions. These results were consistent with the analyses conducted in previous studies (Figure S3) [25-28]. The analyses confirmed the reliability of our pipeline.
The analysis of these variants revealed that the metastatic samples had high tumor mutational burden (TMB, Figure 1C) and low tumor heterogeneity (MATH, Figure 1D). It showed newly occurred and similar mutations when tumors metastasized to liver, bone, and other organs. The comparisons of the variants between primary tumors and metastases also provided 11 metastasis-enriched features (Figure 1E). They included mutated TP53, SHANK1, AR, KMT2C, RB1, APC, CTNNB1, PIK3CA, ATM, CDK12, and SPEN. Specifically, AR mutations were rare in primary prostate tumors but common in metastatic prostate cancer. KMT2C mutations were significantly high in metastatic samples. Combined with previous studies [26, 29], these results suggested the 11 features as potential metastatic drivers. All the above results revealed the genomic heterogeneity between primary and metastatic prostate tumors.
Moreover, genetic differences existed not only between primary tumors and metastases but also among diverse distant sites of metastases from prostate tumors. Specifically, the MATH value of lymph node metastases was the highest compared to other metastatic sites (Figure 1D). This observation may indicate that a portion of the metastases involved lymph nodes as nodes of dissemination. And the lymph node metastases had more variants (Figure S4), suggesting a higher degree of genomic instability and molecular alterations contributing to the metastatic process through lymph nodes. Additionally, the gene of AR was frequently mutated in lymph node metastases (22%, Figure S4B) and bone metastases (18%, Figure S4C). It may describe the potential roles of AR mutations in the progression of bone and lymph node metastases. These results highlighted the diverse mutational profiles and genetic heterogeneity across different metastatic sites. (emphasis added)
* * *
Full paper link:
Heterogeneity and genomic evolution of metastatic prostate cancer, bioRxiv Preprint, Posted September 04, 2023.
Very interesting to see the specific mutations most identified in PC metastases in section 3.1. Some of the mutated genes may be targetable to some degree. From a more global perspective it re-emphasizes the importance of reducing the ongoing accumulation of mutations, "genetic instability". This requires two elements: DNA damage, and growth, the replication of cancer cells forming new variants of populations capable of treatment resistance, androgen independence, immune evasion, invasiveness, etc. Navigating those waters is the adaptive challenge as it is always evolving. Thanks for posting. Paul
Do you know whether the somatic mutations were from treated patients (versus mets at diagnosis)?
My early PubMed reading (19 years ago) included studies where researchers were looking at the AR for something that might explain why cancer had occurred. The AR at diagnosis was usually "wild type".
{However, there was great interest in CAG repeats:
1997:
"We conducted a nested case-control study of 587 newly diagnosed cases of prostate cancer detected between 1982 and 1995, and 588 controls without prostate cancer, within the Physician's Health Study. An association existed between fewer androgen receptor gene CAG repeats and higher risk of total prostate cancer [relative risk (RR) = 1.52; 95% confidence interval (CI) = 0.92-2.49; P trend = 0.04; for men with CAG repeat lengths or = 26 repeats]. In particular, a shorter CAG repeat sequence was associated with cancers characterized by extraprostatic extension or distant metastases (stage C or D) or high histologic grade (RR = 2.14; CI = 1.14-4.01; P trend = 0.001). This association was observed individually both for high stage (RR = 2.23) and high grade prostate cancer (RR = 1.89). Men with shorter repeats were at particularly high risk for distant metastatic and fatal prostate cancer."
There were studies that looked at (unmatched) AR at diagnosis versus AR in CRPC. And even one study that actually had before & after tissue for some men.
There was also data obtained from metastatic tissue after death, following resistance to androgen ablation.
I don't recall there ever being tissue from mets at diagnosis, so I suppose I came away with the idea that somatic mutations were treatment-induced.
In the absence of treatment, PCa in the prostate might have very little evolutionary pressure to mutate. The same isn't necessarily true for cells that migrate, of course.
Anyway, I was fairly confident when I started to use testosterone continuously, since I did not expect the AR to be mutated. I did expect changes in the ERalpha:ERbeta situation, so used an aromatase inhibitor. I did not use a 5AR inhibitor since there was no reason to suppress DHT at that point. Eventually, when the PSADT started to shorten, I used Avodart.
I got a number of years out of this before I needed to consider an AR-axis inhibitor. So far, periodic use of T seems to have reversed AR adaptations.
I do have spinal mets that have been treated with radiation (except a small lesion at S1) and I would be interested to know how they had to adapt to that environment.
It's a concern that I have PSA under control & yet the occasional spinal met has not responded as well. The need for radiation seems to me to be a failure of my protocol.
So am I to understand that you were on continuous testosterone (SPT) for some extended period then added 5ARi when PSA rise accelerated? I would not use continuous T because it induces compensatory decline of AR activity and number, since the system is highly regulated. And high AR expression/activity is a predictor of better response of SPT reducing PCa growth. (More favorable responses to BAT) So periodic cycling to androgen deprivation ADT and an ARSI which causes fairly rapid rise in AR number and activity. Thus restoring sensitivity in preparation for the next high-T cycle. What I do not know is how rapidly these adaptations take which would better guide cycle lengths in BAT programs. Currently I am doing 3 months of high T, keeping above 1000mg/dL continuously, then one month of ADT AR blockade with Orgovyx plus Darolutamide. ADT monotherapy is inferior to combined with an ARSI to limit replication and hence mutations. And Darolutamide appears particularly robust in this regard.
Sorry to hear about the spinal mets, Patrick. But good to have the SBRT as a backup when needed. So we adapt and evolve our best-laid battle plans as their inevitable imperfections become revealed. Paul
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.