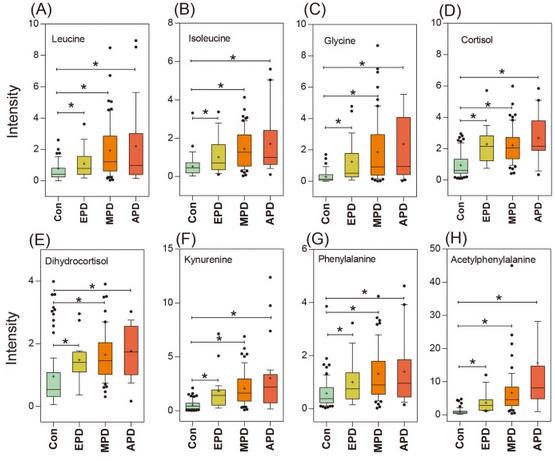
Box plot showing levels of representative metabolites in normal controls (CON), early-stage PD (EPD), mid-stage PD (MPD) and advanced-stage PD (APD).
(A) leucine, (B) isoleucine, (C) glycine, (D) cortisol, (E) dihydrocortisol, (F) kynurenine, (G) phenylalanine; (H) acetylphenylalanine. Asterisk(*) denotes P < 0.05. A cross (+) denotes the mean value of the data.
====================
So I was circling back to see if I should reconsider Glycine for my stack. I removed it quite awhile back. Generally what I find is a Glycine re-uptake inhibitor is something being talked about. I think a re-uptake inhibitor would lower your Glycine.
Then I found this, and it shows how PwPs Glycine level keeps rising the worse they get. This makes sense, considering my previous post on how higher Glycine levels enable Homocysteine to damage neurons: healthunlocked.com/cure-par...
This is very interesting, thanks for posting. Since metabolism is so complex it is difficult to know what effect glycine supplementation would have on someone with PD. Perhaps the extra glycine is the result of protective mechanisms for reducing effects of neuroinflammation caused by the disease. Or perhaps it is just a byproduct of metabolism gone awry and adding more would cause excitotoxicity. The only way to know would be to run an experiment.
Yes, I considered that the excess Glycine might be an effect of some other action, but that other article explaining how Homoceistine can't damage cells nearly as much without elevated Glycine levels puts me on the side of trying to get Glycine levels down to normal. There is also the fact that when people do talk about Glycine for PD, they talk about Glycine re-uptake inhibitors (which I think would lower Glycine, but I am not 100% sure).
Tri Methyl Glycine / TMG / Betaine reduces homocysteine and also restores methylation particularity for those supplementing with niacin or other NAD precursors.
The potential benefits of nutritional homocysteine control are great, while the dangers are virtually nonexistent. Based on the weight of accumulated evidence, our clinic advocates lowering homocysteine levels above 7-8 µmol/L using a graded dosing of three B vitamins, up to maximum doses of 5000 mcg of folic acid, 100 mg (occasionally even 500 mg under a doctor’s supervision) of vitamin B6, and up to 1000 mcg of vitamin B12. Our treatment goal is to lower homocysteine to below 7 µmol/L. We also advocate using choline and trimethylglycine (TMG or betaine) from food or nutritional supplements to augment the benefits of B vitamins and to more effectively suppress the after-meal surge in homocysteine that is not fully controlled by vitamins alone.
Your choices for controlling homocysteine include:
• Folic acid. Folic acid is the most important factor in controlling homocysteine. Although the US recommended daily allowance (RDA) for adults is only 400 mcg,47 extensive survey data showed that an extraordinary 88% of US adults have a folic acid intake below the RDA.48 Low folic acid intake by pregnant women carries a particularly dire risk, causing devastating neural tube defects in newborns. Low folic acid intake from diet is a growing problem because of food processing. This prompted the FDA to mandate folic acid fortification in enriched grain products.
Fortification provides an estimated extra 100 mcg of folic acid daily for most adults and does indeed result in modest reductions of about 0.5 µmol/L in homocysteine. Nonetheless, obtaining sufficient quantities of folate (the food form of folic acid) from foods is difficult, and the majority of Americans not taking folic acid supplements have sufficiently low blood levels that allow higher homocysteine levels.49 Keep in mind that folic acid supplements are twice as bioavailable as folate from food.50 For example, 200 mcg of a folic acid supplement (as an individual supplement or added to grains) provides the same active quantity as 400 mcg of naturally occurring folate from food.51 If you do not eat grain products or you have a higher level of homocysteine, specific folic acid supplementation beyond that in your diet will be necessary. A daily folic acid dose of 800 mcg may lower homocysteine by around 25%.52-53 However, some doctors prescribe folic acid doses up to 5000 mcg for highly elevated homocysteine levels.
• Vitamin B12. Vitamin B12 deficiency is common and can contribute to rising homocysteine, particularly in people over 65. In rare cases, replacing folic acid alone can mask a latent B12 deficiency, resulting in nervous system disorders.
As a general rule, vitamin B12 and folic acid should be replaced together to maximize their homocysteine-lowering effects. Absorption of B12 is a little tricky, and in the past, physicians simply injected B12. However, more recent data suggest that a dose of 500-2000 mcg is every bit as good as an injection.54 A recent dose-exploring trial established that even 500 mcg of B12 achieves the same effect in correcting B12 deficiency as injectable forms. If you are not B12 deficient (discuss this with your doctor), then lesser doses are sufficient. Our clinic commonly advises patients to take 250 mcg of B12 along with folic acid, a dose that provides about two thirds of the effectiveness of the higher doses.54
• Vitamin B6. Taken along with folic acid, vitamin B6 is effective in blocking post-meal surges of homocysteine, particularly when methio-nine-rich meats are part of the meal. Low blood levels of B6 are common, especially in people with higher homocysteine levels.55 The precise dose of B6 required for maximum homocysteine lowering has been controversial, with doses of 2–50 mg commonly used in clinical studies. However, Dutch researchers who have extensive experience with homocysteine-lowering therapies routinely use 250 mg of B6 without ill effect.43,56,57
High-dose vitamin B6 (100-500 mg per day) has been used successfully in managing perimenstrual symptoms and carpal tunnel syndrome.58 However, in rare cases, higher doses may cause nervous system dysfunction (peripheral neuropathy).58 Most reported cases of neuropathy associated with vitamin B6 supplementation involved intake of 500 mg or more daily for two years or more.59 Vitamin B6 doses higher than 100 mg should therefore be used only under medical supervision. The vast majority of people obtain substantial homocysteine-lowering effects with 50-100 mg per day, provided folic acid is at optimal levels.
• Trimethylglycine (TMG). Also commonly known as betaine, TMG is a constituent of food. The average American ingests 500–2000 mg of TMG a day. Supplemental TMG reduces homocysteine starting at a dose of 1000 mg a day, up to a maximum 20% reduction at 6000 mg per day, the dose often used in severe homocysteine disorders.60
TMG is the most effective nutritional agent for suppressing the after-meal surge in homocysteine, slashing levels up to 50%.60-62 We commonly use 2000 mg per day as a starting dose for fasting homocysteine levels that do not fully respond to the three B vitamins, using higher doses for the after-meal surge seen with methionine loading. Spinach and wheat germ are two particularly rich food sources of TMG. Be aware that the 6000-mg dose of TMG has been found to raise LDL by around 10%,63 and LDL should therefore be monitored when using this high dose of TMG.
• Choline. Choline is directly converted to TMG in the body. Choline is readily available in various foods and also as a nutritional supplement. Most people ingest 300-1000 mg a day from dietary sources. Choline has recently gained acceptance as an essential nutrient. To avoid deficiency states, the National Academy of Sciences and the US Institute of Medicine recommend a daily intake of 550 mg for men and 425 mg for women. Higher doses are required to obtain the full benefit of lowering homocysteine. Like TMG, choline has modest effects on fasting homocysteine and a larger effect on the after-meal surge of homocysteine.64 A common dose is 2000-4000 mg per day.
• Avoiding methionine-rich foods. Methionine is an amino acid found in food, particularly red meats and dairy products. Although methionine is an essential amino acid, it is also suspected to cause atherosclerotic plaque growth, both directly as well as indirectly by increasing homocysteine levels.65 The US RDA for methionine is 900 mg a day, but the average American takes in a greater quantity of around 2000 mg a day.37 If excess methionine is available in the diet, more homocysteine is produced. This provides the basis for one of the tests for hidden homocysteine excess, the “methionine-loading” test. The after-meal surge in homocysteine is prevented by vitamin B6 availability, along with choline and TMG.
• Fish oil. Along with its other remarkable benefits such as lowering triglycerides, reducing fibrinogen, and stabilizing abnormal heart rhythms, fish oil may lower homocysteine. Homocysteine reductions of 36-48% have been reported,66,67 though practical experience suggests a more modest drop of 1-2 µmol/L can be expected.
• Taurine. This amino acid and byproduct of methionine metabolism is emerging as a promising agent for reducing the dangers of homocysteine.68 However, further human data are needed to assess its effects.
• Exercise. In a cardiac rehabilitation program following bypass surgery, angioplasty, or heart attack, 76 participants experienced a modest 12% reduction in homocysteine just by engaging in a modest program of regular exercise. How or why exercise results in such a reduction is unclear, but this is yet another example of how physical activity yields broad health-promoting benefits.69 "
More on Homocysteine: Serum Homocysteine Level in Parkinson's Disease and Its Association with Duration, Cardinal Manifestation, and Severity of Disease 2018 ncbi.nlm.nih.gov/labs/pmc/a...
It seems we don't all have high homocysteine levels, just about 20% of us, but our level are higher than non PwP:
"Results
The mean level of serum homocysteine in case and control groups was 14.93 ± 8.30 and 11.52 ± 2.86 µmol/L, respectively (95% CI: 1.68; 5.14, P < 0.001). In total patients, 85 had normal serum homocysteine level, while 15 had high serum homocysteine level. In controls, the homocysteine level was 98 and 2, respectively (P=0.002). In multivariate logistic regression analysis, serum homocysteine level higher than 20 µmol/L was accompanied by 8.64-fold in Parkinson's disease involvement (95% CI: 1.92; 38.90, P=0.005).
Conclusion
Increasing serum homocysteine level elevates the rate to having PD. Serum homocysteine levels did not have any relationship with the duration of the disease, type of cardinal manifestation, and the severity of Parkinson's disease."
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.