Immunoglobulin M (IgM), which is found mainly in the blood and lymph fluid, is the first antibody to be made by the body to fight a new infection. Does IgM tend to be remain low as a result of taking Rituximab [Rituxan] or other CLL drugs?
Are there any known drug or nutraceutical [nutritional supplements] remedies for elevating IgM back to normal levels?
Higsby
Written by
Higsby
To view profiles and participate in discussions please or .
I do have CLL - since 2012? My IgM is very low, but the other immunoglobulin levels are slightly low.
I am not experiencing a lot of infections. However, I do take a lot of herbals, such as Chinese mushrooms, oil of oregano caplets, olive leaf extract, etc.
All CLL treatment drugs target B-cells, both CLL and healthy ones. B-cells normally mature into our immunoglobulin 'factories', plasma cells, so therefore any CLL treatment would be expected to impact our IgM, IgA, IgG, etc, at least while under treatment. Some of the newer, non-chemo drugs are a bit more selective in targeting CLL preferentially over healthy B-cells, such as Venetoclax and perhaps the BTK inhibitors such as Ibrutinib, but recovery of our immune system after successful treatment remains a challenge.
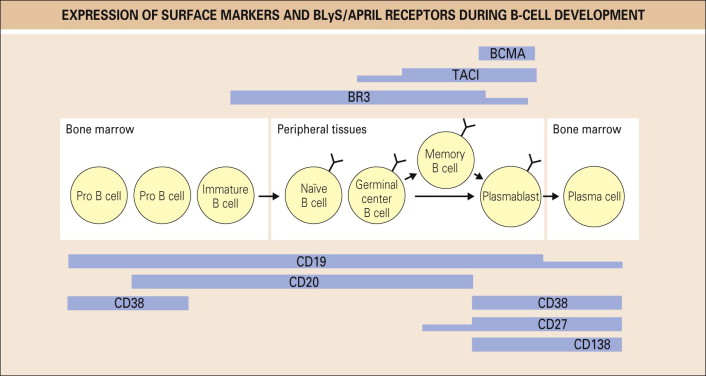
With regard to your question about Rituximab in particular, (or for that matter, any CD-20 monoclonal antibody, which now includes Obinutuzumab/Gazyva and Ofatumumab/Arzerra (both FDA approved for CLL treatment) and Ublituximab (yet to be approved), I've taken the liberty of adding an image from section 4, Principles of Management from Rheumatology (Sixth Edition), 2015, by Edward M. Vital, Shouvik Dass and Paul Emery. You can see that these Monoclonal Antibody drugs (hence the mab suffix) selectively target B-cells other than at the beginning and end of their life cycle. Pro B-cells (i.e. B-lymphocyte stem cells) and plasma cells should not be targeted. So theoretically, once you cease Rituximab treatment, your B-cell life cycle should eventually recover along with your immunoglobulin counts. The problem is that once you have wiped out all the B-cells, there is nothing for the remaining Rituximab to target, so it remains in your blood stream for a long time - upwards of 6 months to a year after your last infusion, wiping out new B-cells until all the Rituximab has been exhausted. Only then can you start on recovering your immunoglobulin production.
My oh my! I never did understand the apparent negative-impact of the residual Rituximab upon the extended half-life of the Rituximab ~~ 'till now (viz. "The problem is that once you have wiped out all the B-cells, there is nothing for the remaining Rituximab to target, so it remains in your blood stream for a long time - upwards of 6 months to a year after your last infusion, wiping out new B-cells until all the Rituximab has been exhausted. Only then can you start on recovering your immunoglobulin production.")
Just to reaffirm the feedback you've received from those with low immunoglobulins despite not having had treatment, hypogammaglobulinemia is a well-recognized complication in chronic lymphocytic leukemia (CLL). It's prevalence at the time of CLL diagnosis is explored in this paper.
Note: "Of 1103 CLL patients who had a normal IgG at diagnosis and who did not receive CLL therapy, the risk of acquired hypogammaglobulinemia was 11% and 23% at 5 and 10 years, respectively".
This paper notes that "Chronic lymphocytic leukemia (CLL) is characterized by progressive hypogammaglobulinemia that can affect one or more immunoglobulin subclasses".
Both papers concur that "The presence of hypogammaglobulinemia does not appear to impact survival."
Finally there aren't "any known drug or nutraceutical [nutritional supplements] remedies for elevating IgM back to normal levels". The standard approach is to monitor immunoglobulin levels during the course of CLL and prescribe infusions of IgG if IgG counts drop sufficiently low and regular severe infections are experienced. There is no way to boost IgM, but the IgG assists somewhat. IVIG tends to be done every 4 weeks or longer, and subcutaneous IgG tends to be done weekly. You get quite large peaks and troughs with IVIG, because IgG has a half life of about 22 days. Subcutaneous IgG smooths out the blood serum levels, both because of the more frequent infusions and because it diffuses gradually out of the infusion site into the blood stream over the following week.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.