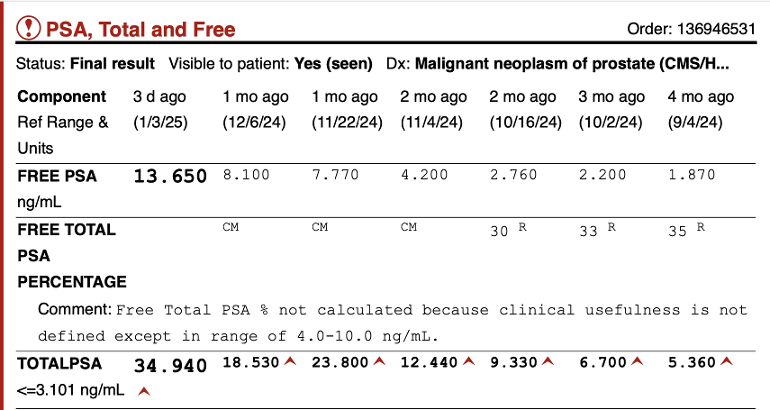
PSA from the day before 3rd 400mg Testosterone shot on Transformer Trial shows a continued rise from 12.4 to 34.94. Is this considered a failure? A certain amount of PSA rise was anticipated due to the increased rise in testosterone and I'm trying to take it all in stride. But what is the cutoff point with PSA rise where we push the alarm button?
BAT failing? Danger zone?: PSA from the... - Advanced Prostate...
BAT failing? Danger zone?
Written by

SViking
To view profiles and participate in discussions please or .
Read more about...
39 Replies
•
When PSA is growing exponentially, you can be sure the testosterone is fueling cancer growth. BAT can be dangerous stuff.
When Psa increased from <.014 to .04 in 4 months. Does this increase considered “growing exponentially”? Thanks.
No. Below 0.1 does not count.
i would jump right back on ADT and hopefully it drops. It should if your cancer is androgen dependent. That’s what BAT can do is sensitize the cancer to androgen then knock it back down with ADT. Everyone is different and we each have different levels of oh crap values. Look at my posts on my BAT story. You will see a jump in my PSA values and then a rapid drop after going back on ADT. It is a balancing act and remember the idea is to keep the cancer androgen dependent so you can go back and forth.
I understand your point. But it’s also my understanding that in some cases after a few months on BAT while continuing on ADT that there’s a chance PSA will drop. Then it could start to rise again. An initial rise was anticipated. My question is how far to let the PSA rise before starting second generation again. In my case that would be Nubeqa.
That is a difficult question to answer and it would either be up to you and your oncologist or just you. Are you in a trial?
yes. I'm in the transformer trial but there may be other options.
So reading the trial are you done with it? I take it you are using enzalutamide.
What are your other options?
I’m trying to figure out if I’m done with it or not. In some cases it calls for a 400mg testosterone shot every 28 days for three months. But other circumstances appear different. It seems some guys are doing the shot every other month for several years. Their PSA appears low and steady.
As per transformer trial, I stopped Nubeqa during this waiting time Still waiting for reliable opinions on options.
Well if you stopped nubeqa, you’re outside of trial. I definitely wouldn’t… wait a minute i thought the Transformer trial was with enzalutamide?
I am confused
Good question. As I suspect you know, at a biochemical level T is increasing synthesis of PSA while causing PCa to differentiate and slow proliferation. At least this is what the lab models show and is what this approach predicts. Thus PSA ceases to be a reliable marker of tumour load.
What other measure of tumour load is being used? Has a repeat PET been done? If it were me and I felt I was improving clinically I would hang in there if your oncologist is confident. Have you addressed this question with your oncologist ? If you have resistant disease do you have anything to lose ?
The final question, for which your oncologist is responsible, is when or whether to restart ADT. I don’t know your trial protocol and this is presumably built into the trial?
Bottom line is that I am not sure anyone here is in a position to give definitive advice and really you should be discussing and challenging your oncologist.
Oncologists aren't all that up on BAT either, unfortunately, as I am sure you have come to know. In fact, I would say you're a lot more up on it than 99% of oncologists. But it does appear that the high T is not working here
"What other measure of tumor load is being used? Has a repeat PET been done?" Now scheduling a fresh PSMA scan to compare with last one a few months ago.
" If you have resistant disease do you have anything to lose ?" Not really. I have been castrate resistant for last two years having failed Zytiga, enzalutimide, Nubeqa, Pluvicto and multiple SBRTs.
"The final question, for which your oncologist is responsible, is when or whether to restart ADT. I don’t know your trial protocol and this is presumably built into the trial?" The problem is that few oncologists approve of, or understand BAT. Even Dorf at City of Hope has no experience with it--only what's on the Transformer literature. She agreed to it at my request. It's my understanding that there are a variety of BAT besides Transformer. Mix and match with Chemo, Radium 223 or?
quick follow-up. Just seen summary of the Transformer trial phase 2. So you must be in a new trial??
Not sure which phase.
Be interested to see what your T levels are as well, during those PSA screens.
Wondering if a PET scan or any other imaging is used in conjunction with the BAT therapy as well, let alone with the climb in PSA.
BAT for some, is and can be basically playing Russian Roulette... Especially if in the advanced stages of PCa.
Wishing you the Best of Luck & Regards
but do you feel better? 😀 Quality of life is one of the things they include in the notes now, I have noticed, not just survivability.
Hi. Good question. 😀 You may well be right. For me QOL beats quantity.
those are significant doubling times and concur with the other comments on pet PSMA scans and I would request other circulatory blood test to be done so you can see where you start and end. Meaning there’s a bone specific alkaline phosphate BAP. It it would give you a start point and an endpoint for where you’re at in the last four months so along with the PSA it’s an indicator of micro metastasis. If the PSAPET scan threshold can’t pick those up. potential bone metastasis. Being in a research setting, you should be requesting these things even if they don’t tell you.. for your own safety . Even at this point, I would still request a BAP. And assuming if this is the properly run trial, you should already be ADT. You may possibly need to change the flavor of the ADT MECHANISM OF ACTION. Meaning eligard /Lupron or whatever the study is controlling.
As tall Allen said BAT is risky sensitization protocol. I don’t believe they do very thorough Gene mutation vetting therefore you can have the responsible set of gene mutations that respond to this and in a whole bunch that don’t and then add on the specific cell lines are really replicating fast. I struggle to find this info and if anybody has it would love to see some and share it with us all.
Thanks. Can you recommend specific things to test for at next blood test? Biopsy? Currently still on Orgovyx.
Guardant 360 blood. That’s the circulatory mutations test that can be done without a biopsy. If you’ve already had a biopsy, they should be able to pull your samples. That are required by law to be saved in Cryro. So either source you can get genetic testing done. This will allow you to know what gene mutations will respond to targeted therapy, such as parp1 inhibitors or immuno therapies. Also the BAP test, because PSA alone is an indicator not a diagnostic. At least with the BAP you can see if PSA is increasing while monitoring bone met activity.
this Group here has a lot of information on additional ancillary tests available.
I broadly agree with Eieio. As he says we do not know whether all mutant variants respond in the expected way to high levels of T.
On the risk side the data so far from the Transformer phase 2 trial showed BAT was safe and associated with better QOL (approx 100 patients in each arm). The switching from BAT to Enzalutamide showed better results than the other way round. I have copied the data from the abstract:
Overall survival was 37.1 months for patients crossing from BAT to enzalutamide versus 30.2 months for the opposite sequence (HR, 0.68; 95% CI, 0.36 to 1.28; P = .225). BAT adverse events were primarily grade 1-2. Patient-reported QoL consistently favored BAT.
Conclusion: This randomized trial establishes meaningful clinical activity and safety of BAT and supports additional study to determine its optimal clinical integration. BAT can sensitize CRPC to subsequent antiandrogen therapy. Further study is required to confirm whether sequential therapy with BAT and enzalutamide can improve survival in men with CRPC.
I note Eieio suggests checking bone specific alkaline phosphatase but another (perhaps old fashioned but still useful enzyme) is acid phosphatase which is still sometimes used to monitor PCa tumour load.
I dont think we know enough about the protocol SViking is following to really comment sensibly, and I do think he needs to pin the oncologist down rather than relying on us amateurs!! Best wishes to SViking.
Maybe it's time to return to Nubeqa. I guess we will decide after next blood test and PSMA scan. And I receive far more discussion here than with doctors. Thanks to all of you.
Hi SViking. I am beginning to understand your predicament more clearly. It seems to boil down to the fact that your Onc does not know what they are doing!!
If you are in a trial, and I am still not certain about this, ask the Onc to show you the protocol you are following which should specify the outcome measures being used and what the criteria are for stopping etc.
There are some comments here which seem not to understand BAT. The whole point of BAT is to resensitise the tumour cells with T in someone no longer ADT responsive. So you cycle between T and the ADT starting with T to wake the PCa cells up.
Finally if your Onc does not understand the therapy they should put you in touch with an Onc who does AND show you the protocol you are following. It sounds somewhat unprofessional leaving you swinging in the wind.
Thanks again. I tried to schedule a Zoom appointment with Dr. Denmeade the lead investigator and primary proponent of BAT but he is at John Hopkins in Maryland and can't do Zoom with out-of-state patients. To be fair with my Onc here, there is not much data yet to review.
I don't think you can determine if BAT is failing unless you analyze both sides of the coin. You are only presenting PSA results based on half the BAT treatment. What your PSA does when you switch back to ADT will answer your question I would think.
When you get BAT you continue your ADT. Otherwise the testosterone would not return to castrate levels: "all patients should continue to receive concurrent ADT throughout treatment with BAT, and ADT should not be stopped when BAT is administered." pmc.ncbi.nlm.nih.gov/articl...
Does that assume that BAT is only for castrate resistant metastatic PCa? And if it is castrate resistant, why would they continue using ADT? I mean, if it does no good. But I do see in the article very clearly they state to continue taking it but if you are taking injectable T I wouldn't think your testes would produce much anyway
Thanks. But given that the last time I went off of Orgovyx it took four month for T to even begin returning maybe a short break would help. So if ADT only serves to lower T, if I temporarily stopped Orgovyx would that really make a difference in BAT?
ADT only serves to lower T. But lowering T serves to stop non-resistant cancer cells from growing. Even if you are castrate-resistant, not all cancer cells are resistent and lowering T shall serve to stop these from growing. One can look at it the other way, if your T does not recover, what do you gain from stopping Orgovyx during your BAT therapy?
I have no knowledge how the PSA value should develop during a BAT therapy in your case, but I have the impression that a PSA of 35 ng/ml should get you to discuss this with your doctors.
I had a PSMA scan done yesterday and will do blood work tomorrow. Stay tuned! And thanks so much for all those who are contributing to my questions.
Ask Denmeade himself but if you have bone Mets and you doctor is not monitoring alp as well as Psa you need another oncologist. Denmeade requires face to face for first visit no matter where you live even if he is licensed in your state. Send him an email.
X
Thanks. I'd love to visit Denmeade but flying from So Cal to Hopkins does not work for me at this time.
I’m in SoCal. Denmeade requires a personal appearance at Hopkins. Not feasible for another month anyway.
Not what you're looking for?
You may also like...
DIY BAT
G’day
I thought it might be useful if I briefly described my experience with Bipolar Androgen...
Hormone Therapy failing?
Hi all,
My father was diagnosed with PC in Nov 2017, Gleason 4+4 PSA 12 and had is prostate...
BAT trial
With Xtandi failing and my metastasizes not PSMA avid enough for Lutetium my MO referred me to the...
My first month of BAT therapy
So here are the figures for my first month on BAT therapy
DAY 1 PSA 5 testosterone castrate level...
Docetaxel Failing
Greetings from Inverness in the beautiful Highlands of Scotland! I would like to share my journey...