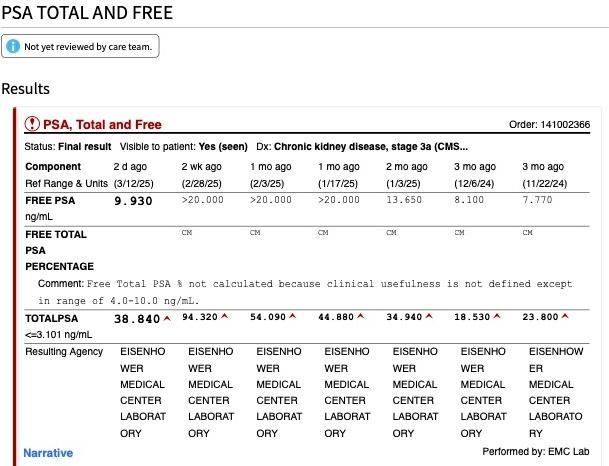
After four months of BAT with monthly shots of 400mg testosterone I started up again with Nubeqa. Original PSA before starting BAT was 12. 4 and ended with 94.32. Twelve days later first PSA number dropped from 94.32 down to 38.84. I'll get another PSA test in two more weeks. Hopefully it trends down non-detectable.
What do you guys think?
Written by
SViking
To view profiles and participate in discussions please or .
UCLA ONCOLOGY IMAGING PET CT BODY WITH DIAGNOSTIC CT OF THE NECK CHEST ABD PELVIS W/IV CONTRAST 01/15/2025
PURPOSE OF PET/CT: Localization of Biochemical Recurrence.
ORDER INFORMATION PER REFERRING PROVIDER: rising PSA.
CLINICAL HISTORY PER EMR: History of metastatic prostate cancer status post multimodal therapy including radiotherapy to multiple sites, PSMA PET 8/19/2024 with new sites of disease, started on relugolix.
TECHNIQUE: Imaging was performed on a Siemens Multidetector PET CT Scanner. A single volume noncontrast CT of the upper abdomen was acquired in quiet breathing. After the administration of intravenous contrast, volumetric CT scan of the chest was obtained in full suspended inspiration, and reconstructed at 1 mm and 3 mm. Thereafter, volumetric CT was acquired from the top of the skull to the knees. After a standard uptake period following radiotracer injection, PET images were acquired, using multiple positions along the same length of the patient's body as the CT. Iterative methods were used to reconstruct the PET images with a slice thickness of 5 mm. The CT images were used for attenuation correction. Additionally, delayed images of the pelvis were acquired. Oral hydration with 1 liter of water was given. Oral contrast was administered prior to the examination.
Contrast and Radiopharmaceutical: gallium Ga 68 gozetotide inj 5.95 millicurie diatrizoate meglumine-sodium (MD-Gastroview) 30 mL in water 1000 mL oral soln iodixanol (Visipaque) 320 mg/mL inj 100 mL
Radiopharmaceutical uptake interval: 97 minutes
RADIATION DOSE: The patient received the following exposure event(s) during this study, and the dose reference values for each are as shown (CTDIvol in mGy, DLP in mGy-cm). Note that the values are not patient dose but numbers generated from scan acquisition factors based on 32 cm (L) and/or 16 cm (S) phantoms and may substantially under-estimate or over-estimate actual patient dose based on patient size and other factors. CT Abd wo, CTDI(L): 9.7, DLP: 381.3;CT LungAbd w, CTDI(L): 9.6, DLP: 537.3;CT WB, CTDI(L): 8.4, DLP: 1143.6;ACCT PLVS, CTDI(L): 3.7, DLP: 133
ONCOLOGIC FINDINGS:
History of metastatic castrate resistant prostate cancer status post prostatectomy and radiation therapy with:
-Few scattered new foci of low to intermediate PSMA expression within the osseous structures, for example:
Left humerus, SUV max 5.1 (4-408)
Inferior T1 vertebral body, SUV max 5.2 (4-352)
Right lateral seventh rib, SUV max 3.5 (4-280)
Right T7 transverse process SUV max 2.7 (4-311)
-Interval decrease/resolved PSMA expression within the previously described osseous structures including the clivus, cervical, thoracic, lumbar spine, left iliac bone, scapula, humeri, and ribs, for example right clavicle with associated sclerosis current SUV max 2.1 (4-354), 8/19/2024 = SUV max 10.4 (4-152). Additional sclerotic osseous lesions without PSMA expression compatible with treated disease.
-Slight increase in the low PSMA expression within the right retrocrural region, nonspecific.
-Mild bilateral gynecomastia with resolved PSMA activity on the left.
ADDITIONAL FINDINGS:
PET:
Physiologic PSMA uptake is noted in the lacrimal and salivary glands, nasopharynx, vocal cords, gastrointestinal tract (especially duodenum), spleen, liver, both kidneys, ureters and the urinary bladder, and testes.
Lungs: Unchanged bilateral lower lobes reticular scarring and atelectasis.
Lymph nodes and Mediastinum: Ovoid calcified lesions in the anterior mediastinum, stable.
Pleura: Left upper lobe calcified pleural plaque, unchanged.
Cardiovascular: Mild to moderate atherosclerotic calcifications of the thoracic aorta and coronary arteries. Left superior vena cava,draining into coronary sinus.
ABDOMEN/PELVIS:
Liver: Stable punctate calcification in the caudate likely represents a prior granulomatous disease.
Gallbladder and bile ducts: Unremarkable.
Spleen, pancreas, adrenals: Stable punctate calcification in the spleen likely represent prior granulomatous disease. Unchanged mild prominence of the main pancreatic duct.
Kidneys and ureters: Atrophy of left kidney with scarring and mild hydronephrosis. Stable left renal cyst.
Bowel: Scattered colonic diverticula.
Bladder and reproductive organs: As above.
Lymph nodes: Unremarkable.
Peritoneum: Unremarkable.
Vessels: Mild to moderate atherosclerosis.
Abdominal wall: Postsurgical changes in the anterior abdominal wall. Status post bilateral inguinal hernia repair.
MUSCULOSKELETAL:
As above.
Multilevel degenerative changes of the spine.
Degenerative changes of the shoulders with small right joint effusion.
Chronic rib fractures involving the right posterior fifth and sixth ribs.
Retention sutures in the left proximal humerus.
Stable L5 spinous process hardware in place.
Trace to small right and trace left knee effusions.
IMPRESSION:
History of metastatic prostate cancer with mixed response to therapy including decreased/resolved PSMA expression of the previously described osseous lesions with new foci of low to intermediate PSMA expression within the osseous structures since 8/19/2024.
intravenously. In line with the clinical standards of practice, the
patient' s blood glucose was measured in this office prior to injection at 115 mg/dl.
In addition to transverse plane images, coronal and sagittal reconstructions
are created and reviewed for the CT and PET images. Oral contrast was
administered prior to the exam.
FINDINGS:
Background activity in the mediastinal blood pool: SUV max 2.3
Background activity in the liver parenchyma: SUV max 3.2
Please note, the sensitivity of this unenhanced, nondiagnostic, low-dose
whole-body PET/CT scan is suboptimal for demonstrating small soft tissue
nodules, lymph nodes, brain metastasis as well as evaluation of abdominal
viscera.
HEAD AND NECK:
On the nondedicated brain images there is no gross FDG-avid lesion,
however, PET has low sensitivity for detection of intracranial metastatic lesions due
to high physiologic background FDG activity.
Paranasal sinuses are unremarkable.
Physiological radiotracer uptake is seen in oropharynx and salivary
glands.
No radiotracer avid cervical lymphadenopathy.
Normal distribution of radiotracer in the thyroid glan
CHEST:
No radiotracer avid lymphadenopathy in the axilla, mediastinum, or bilateral
hilar regions.
Normal sized heart. No pericardial effusion. The thoracic aorta is normal in caliber.
Chest wall is unremarkable.
No abnormal FDG avid lung nodule or consolidation. Bilateral lower lobe subsegmental atelectasis.
There is no pleural effusion.
ABDOMEN AND PELVIS:
Liver and spleen are normal in size without abnormal radiotracer uptake.
No abnormal FDG uptake noted in gallbladder, pancreas and adrenal glands.
Physiological tracer uptake in kidneys and bladder. Redemonstrated mild
left hydronephrosis. Bilateral renal hypodensities..
Redemonstrated subcentimeter bilateral retrocrural lymph nodes with
low-grade FDG uptake of SUV max 2.5, stable as compared to prior study without any
distinct PSMA uptake.
Otherwise, no significant radiotracer avid mesenteric, retroperitoneal, pelvic,
or inguinal lymphadenopathy.
Expected physiological tracer activity noted in the stomach and bowel, without
distinct focal activity. Reproductive organs: Status post prostatectomy. No definite focal
increased tracer activity in the surgical site.
MUSCULOSKELETAL:
There are innumerable FDG avid sclerotic osseous lesions scattered
throughout the axial and appendicular skeleton reference lesions include:
Lateral body of the C1 vertebra with SUV max of 11.4 (image 213, series
3), previously PSMA uptake of SUV max 2.2, Uptake in the left scapula with SUV max of 15.8 (image 178, series 3), previously PSMA uptake of SUV max 2.3
Posterior aspect of the right sixth rib with SUV max of 5.3 (image 148, series
3), previously PSMA uptake of SUV max 2.5,
Anterior aspect of the left iliac bone with SUV max of 4.1 (image 58,
series 3), previously PSMA uptake of SUV max 1.9.
Proximal right humerus with SUV max of 7.9 (image 167, series 3,
previously PSMA uptake of SUV max 2.6
Multiple new areas of increased tracer avidity is noted within the
visualized bones, predominantly in the thoracic vertebrae. Reference lesions
include:
Focal uptake in T3 vertebra with SUV max of 7.9 (image 166, series 3),
Focal uptake in the T12 vertebra with SUV max of 11.8 (image 113, series 3)
Focal uptake in the anterior right iliac crest with SUV max of 7.5 (image 63,
series 3) Few foci of uptake in the proximal right femur shaft with SUV max of 5.2
(image 17, series 3).
Few sclerotic lesions scattered within the visualized skeleton, not demonstrating any significant focal uptake, likely treated lesions.
IMPRESSION:
1. Status post prostatectomy. No distinct focal increased tracer
activity seen
in the surgical bed.
2. Innumerable FDG avid osteosclerotic lesions scattered throughout the
axial and proximal appendicular skeleton, consistent with metastasis.
In comparison to prior PSMA PET/CT, there are new osseous lesions
demonstrating FDG avidity, predominantly involving the thoracic vertebrae, iliac bones and proximal right femur. Previously seen PSMA avid lesions demonstrate higher FDG
uptake (though the PET scans with different radiotracers cannot be compared directly).
Above findings could be seen with poorly differentiated tumor/aggressive tumors/
neuroendocrine prostate cancer expressing low PSMA avidity. Correlate
Due to lower back pain two weeks ago we also had an MRI done last week to see if the pain was from compression fracture, bulging disks or lesions on the bones. Pain passed since though so probably due to bulging disks.
MRI OF THE LUMBAR SPINE WITHOUT CONTRAST
HISTORY:
Pain
M54.50: Lumbar spine pain
COMPARISON:
10/31/2024
TECHNIQUE:
The exam was performed on an advanced high-field MR imaging system. The
following sequences were obtained:
Sagittal T1 SE, sagittal T2 SE, sagittal T2 FSE fat sat, axial T2 TSE,
axial T2
TSE STACK, and coronal T1 SE.
FINDINGS:
Normal conus medullaris is seen terminating at L1. There is no acute fracture or dislocation. There is fatty replacement of the L2-S3 bone marrow suspicious for post treatment changes. There is new focal edema in the right side of T12 and L1 as well as the left side of T12. The remainder of the bone marrow appears unchanged. There is possible left hydronephrosis
L1-2: Disc bulge with bilateral facet osteoarthritis and ligamentum flavum
hypertrophy. Mild central canal narrowing and bilateral neural foraminal
narrowing.
L2-3: Disc bulge with bilateral facet osteoarthritis and ligamentum flavum
hypertrophy. Mild to moderate central canal narrowing. Mild left and
moderate
right neural foraminal narrowing.
L3-4: Disc bulge with bilateral facet osteoarthritis and ligamentum flavum hypertrophy. Mild to moderate central canal narrowing. Moderate to severe right and mild-to-moderate left neural foraminal narrowing.
L4-5: Disc bulge with bilateral facet osteoarthritis and ligamentum flavum
hypertrophy. Grade 1 anterolisthesis. Moderate central canal narrowing.
Moderate bilateral neural foraminal narrowing.
L5-S1: Disc bulge with bilateral facet osteoarthritis and ligamentum
flavum hypertrophy. There are increased left and right paracentral disc protrusions
contacting the descending nerve roots. Mild to moderate central canal narrowing. Moderate right and moderate to severe left neural foraminal narrowing.
IMPRESSION:
1. Findings suspicious for new metastatic lesions at T12 and L1. The remainder of presumed metastatic lesions are unchanged
2. Degenerative changes have advanced, most significantly at L5-S1 where there are new/increased left and right disc protrusions contacting the descending bilateral nerve roots.
3. Presumed posttreatment changes of the bone marrow
4. Possible left hydronephrosis better evaluated on 02/20/2025 CT
A mixed bag to be sure, SV. While I generally like the PSMA results, I don’t like the FDG quote “Above findings could be seen with poorly differentiated tumor/aggressive tumors/neuroendocrine prostate cancer expressing low PSMA avidity”
Still, yer a rockstar doing this your way! “Viking” is appropriate!
Hi add2! Tough question. It would be great if fewer guys ended up in the advanced PCa category.
Here is my take on it and I fully accept that others may well disagree. As a preliminary answer to your question I would select patients on basis of risk at diagnosis. Histology grade etc and I think younger age eg less than 60 maybe, who have more to lose than oldies like me and more likely to have progressive Ca.
The start of a tumour is a single cell (based on studies using X deletions)which quickly develops additional mutations ie becomes oligoclonal. Initially most of those cells are very sensitive to adt and easily eradicated but others not so and so the process of selection starts with the most resistant cells (eg AR duplication, internal T synthesis etc) being progressively selected to survive as a result of adt and receptor blockers .
Here is my speculation. What if we could prevent the inexorable progression of resistance by using BAT to maintain sensitivity to therapy at a much earlier stage???
Anyway I am not in a position to do much about it, but I would like to think there is a possibility of moving on from the relentless T deprivation/blockade model (in which large amounts of money and academic prestige have been invested) which just seems to finish in a dead end. Literally.
Finally the most recent and very large multinational genetic studies have found that risk of developing PCa shows a dose relationship to levels of IGF-1 - whereas T shows no dose relationship. T appears to be necessary but not sufficient for the development of PCa. Food for thought.
A trial I would like to see is on HSPC men. Various grades. Endpoint not only PSA control and rPFS but also time to CRPC.
We had BATMAN but that didn't go far enough.
Cycling needs to incorporate other forms of testosterone or, at a minimum, allow a true ADT state to be entered. Extending cycles would do that. Delicate balance though. Extend them too much and efficacy could be affected.
Yea, I just had a discussion about this with Denmeade. I switched from prednisone to dexamethasone as per Denmeade a week and a half ago hope ago hoping to get a few miles out of that but planning on BAT before chemo.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.