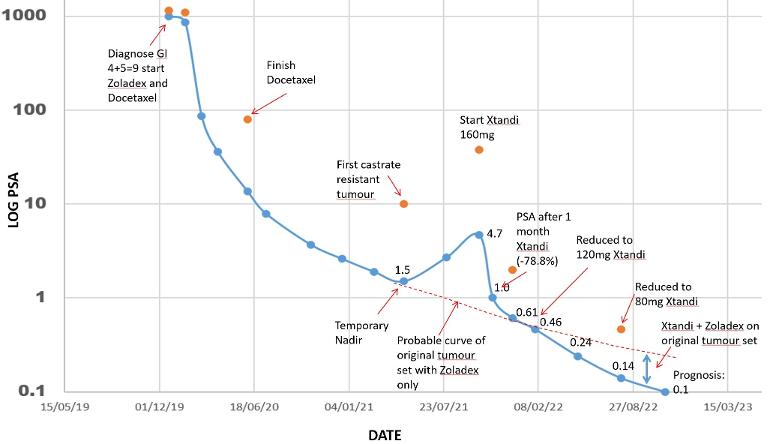
I am always curious about the course of my PCa - which is why I analyse the progression after each 3 monthly reading. Bearing in mind that PSA is not cancer (thanks TA) the smooth and regular nature of the log plot tells me that my PSA in measuring something, and is highly likely to be a reflection of the cancer development, especially the sharpness of the changes linked to the new tumour.. My PC is of the type which gives a strong PSA reaction so I can easily see the progression on the plot.
I always thought of the castrate resistance onset as castrate resistance of the whole tumour set. What I can see from the plot is the castrate resistance outbreak is a distinct new tumour in addition to the original tumour set with its own PSA expression. Also both the new tumour mutation outbreak, and the original tumour set are responding to Xtandi since the downward trend is steeper than the original trend on Zoladex only. Of course if there are also other new castrate resistant tumours which do not have a PSA expression then I will not see them.
Does anybody know if this analysis is in line with the established scientific thinking?
Written by
Stoneartist
To view profiles and participate in discussions please or .
Sorry - its my graph and I know the PSA scale is logarithmic with a base of 10. I dont understand why you should dispute that when you have no information other than what I have provided???
Try to calculate antilog of 1000 on your calculator. You would understand. If your graph shows log of PSA, then 1 corresponds to PSA of 10 and 4 corresponds to PSA of 10000. All I am pointing out the vertical axis is showing PSA not log PSA.
The numbers shown are PSA of course - but they are plotted on a log scale - I thought that was obvious to all. I am sorry if I gave you the impression that the numbers on the scale were log PSA plottet on a log scale - that would indeed be weird. I will amend the scale title to PSA (log scale) if this clarifies things
What was the reason you reduced your Xtandi? I have been on 160MG for 15 months and went from 940PSA to “nadir” .08 so I am similar to your trajectory with PCa. Also did Chemo and continued monthly Firmagon. I guess my MO’s plan is to stay on this regiment until PSA spikes but I am exploring alternatives. Thanks for the graph it’s very helpful.
1. I did some reading and found out that in the original phase trials to test for dosage they tried a range of dosages and that at 180mg and above the side effects became serious. So they seemed to land on 160mg as "safe". but they never tested for minimum amount which remained effective.
2. I read that you reach saturation in the blood after 5 days on 160mg, and it seems logical that remaining at or near saturation should not need such a high dose - like turning the heat down after the water has come to the boil on the stove
3. On this forum there are a lot of guys whose oncologist happily reduced the dose from 160 to 120 or 80 without worry that this would not be enough.
4. It is logical to me that while you might need a high dose to zap the new tumours at the start, it should not need the same concentration to keep the tumours in check thereafter.
So I have tested this on myself and read the results as strong evidence that I was right. Using a smaller dose to do the same job appeals to me as not messing with the body so much - its a fine tuned machine and all medications have the potential to harm more than they help. I am now on 80mg/day.
We are both lucky that we have a tumour type that is high in PSA expression so we can track whats going on.
Very interesting. My advanced hormone is Apalutamide and month 2 has wiped my energy. I will be asking next month about possibility of a reduced dose. Thanks for posting.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.