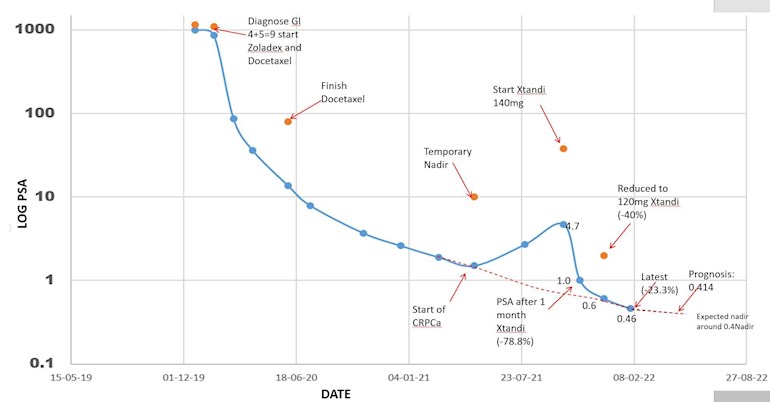
Hi Folks, you may remember I was speculating that the Xtandi dosage was designed in the clinical trials to be at the max possible without incurring adverse side effects. There was little attention paid to the efficacy of the doses. My theory was that while we need a high dose to reach saturation, we can get by with a lesser dose to maintain saturation. This was backed up by my oncologist so I went onto 120mg dose instead of the normal 160mg dose.
48 days later my new PSA value shows a similar reduction to what has gone before suggesting that the 120mg dose was giving a similar effect to the 160mg dose. The curve shows a nice decline - and looks like rejoining the decline curve from the period on ADT alone - as if the castrate resisting cancer was in addition to the previous adt sensitive cancer, and it was quickly zapped by the Xtandi.
Note the plot is on a log scale to emphasize the low values. Looks like I am heading for a nadir of about 0.4 - or just under. This will be just great since I can then follow the PSA changes if I change things that may make a difference - a one man test case-
Written by
Stoneartist
To view profiles and participate in discussions please or .
Nice post. I found the 160 mg dose to be intolerable. 120 mg let me improve. 80 mg dose led me to 3 yrs of near undetectable PSA. I agree with your adt (orchiectomy) holding some in check, xtandi holding second cancer back, and new BCR's have been zapped by RT. Must have at least 3 wonderful mutations at work in my body at this time. Fun. Life Is Good, especially when your treatment gun has all cylinders loaded.
Yes you have mentioned this before - but at this stage I have only the change of PSA value to guide me until the next scan. I read of others with PSA down below undetectable - but that doesnt bother me - I still have a prostate and a nadir of around 0.4 will be just fine. The last scan showed all lymph node tumors gave gone (at least too small to be detected) and the bone metastasis looking like there is growth of new healthy bone material. So now I just keep a steady course on Xtandi and Zoladex and wait for the inevitable sooner or later - preferably later
I have no idea!! Here in Norway the health service picks up the tab - thats why we like paying reasonable taxes - and I believe the health service makes deals with the big pharma companies - so our meds are many times cheaper than in the US. Others may know more about this??
Well - you guys in the US will have to get rid of your fear of socialism before that can happen. Theres a reason that the countries that dominate the top of surveys concerning happiness with life are democratic socialist. That said, PCa doesnt respect these boundaries, which is why this is such a great site
We do need to change the way our elections are financed. Many things might change after that.
Pharma companies in Norway are still private, though, rather than government-owned, correct? Or do I have that wrong. I ask because I think of socialism as government ownership of the actual businesses.
Thats the propaganda you guys get in the US. Most business in europe - including Pharma is private, but the government regulates what they can do so that it is best for society. Things essential to society are often run by the state - hospitals, roads and some places other transport, and sometimes utilities. What you are thinking of is communism - which is a dictatorship in practice - and there I suspect only the rich get to get the expensive drugs - dont go there.
No, I honestly was going not by propaganda, but how the dictionary used to, and still seems to, define socialism: government ownership of major industries. I looked it up after our exchange. Perhaps Europe uses different variations.
We have a lot of regulation here, and many large regulatory agencies, but the regulated industries have far more influence with them than ordinary citizens.
Great Britain was never a communist country, but the government did used to own major industries until selling them off in the 80s. But enough about terminology, and I'm not contending the US medical system is not beset with many problems. I criticize it daily.
Leaving aside how expensive it is, though, and who pays, and how good or bad the care is, does Norway's standard of care differ in any major way? For example, is input on diet and exercise given to patients by doctors? Is the PCa protocol more or less the same, or is something dramatically different?
And I'm still curious about the use of Xtandi vs generic Zytiga. Even in Norway's system, the price differential must be substantial and must catch the healthcare system's attention there. That's why I asked originally. I'm well aware the US system is double the cost of every other medical system. Many want to change it; there just has been no majority consensus about how to do it. I'm sure propaganda does play a serious role.
I honestly dont know how much they cost here in Norway. I pay about $200 of the cost per year - everything over that is free for me.. From what I can see the SOC for prostate cancer here is the same as in the US. They have the same input for diet - eat healthy - we must ourselves delve into the possible effects of different diets if we feel it will help - so basically - not a lot different than what you guys experience. The main difference is I havnt experienced anything like the "shopping for second opinions" here - but my PCa has followed a standard pattern so far - hoping it will continue on its present path.
It's a fascinating discussion. But I wouldn't want you to think that because I ask a few clarifying questions that I am a staunch supporter of the US system. I suspect that all systems have strengths and weaknesses, but not necessarily in equal amounts.
There needs to be a new business model. It's a horrible system in the U.S. because patients many times end up paying much more than overseas counterparts for prescription drugs. Government negotiation and control of drug prices (Ala socialized medicine) seems like an easy answer. Unfortunately, when you take the big money incentives out of the drug business you also lose the pipeline of new and innovative drugs we in the PCa community desperately need. Government negotiated prices are the main reason few novel lifesaving drugs come out Europe. Considering the alternative, I want drugs to be more expensive! It will increase the chances we will finally come up with one to kill the cancer beast.
You must be joking!!! Theres no difference between the US and europe on that - both have more than enough money for research - just look at the profits they make. The " we need money for research" is just a mantra they use to con you into accepting the system,
Research is one thing but bringing a drug to market can cost more than a billion dollars. Two examples illustrate my point HIV and COVID. Only when billions of dollars were directed at HIV was there finally good treatment options (but no cure). Vaccines used to take 7-10 years to develop and get approved. The U.S. and other countries poured billions of dollars into the effort and got approved, pretty good vaccines for COVID in about a year. If we put those kind of resources and incentives (i.e. make it very profitable for the drug companies) into PCa we'd probably have a cure in less than five years. Follow the money
Pfizer Covid vaccine was made in Germany and included a massive subsidy from the government if I am not mistaken, and Astra Zenica followed soon after with one which came from Oxford university made in the UK - so I dont buy your line of thinking. Most of the US people on this site are affected by the cost of medicines, and those without a stash of cash have to rely on medicare. And many have to travel to other places to get the treatment they need. Its heartbreaking to read those stories of fellow warriors.
I'm in total agreement that price should not stop anyone from getting drugs that could prolong or save their lives. We have to keep the cost of medicines in reach of everyone but not kill the future development of amazing drugs. It's a difficult balancing act but I'm glad you're able to get Xtandi in Norway.
Interesting one-person study. I look forward to your this year's results. Where was the bone metastasis? Were your vertebrae, ribs, possibly the skull affected?
I too. didn't like the side effects of 160mg of Xtandi. Dr's were quick to lower dosage to 80mg. PSA has been <1 for 18 months. CT's have shown shrinkage of stage 4 met's. All is well
Thank you very much for posting that graph. I'm a similar trajectory to yours. May 21 PSA 900, palliative radiation, continuous Firmagon and started Xtandi 2 months ago. Current PSA is 6.7, up from 5.7 last month (which is worrisome but MO says I fluctuate some month to month and the trend is down so far.) I've been unable to get any lower than 5.7 and am wondering if there is something else I can do to get it lower?
I’ve been getting Xtandi in addition to Zoladex since August 2021, I feel like a chemical factory. My beard doesn't grow anymore ... I even get the bone protection Xgeva, which makes my jaw very painful. I exist deeply tired, but I still ski😊
Ha Ha - Wouldnt it be nice if it was so - chisel the prognosis in stone and the cancer will follow afterwards - then we could all cure ourselves by meditating , positive thoughts, and living the present. I actually believe there is great power in positive thoughts - and a good dose of tantra-zen!!
You are correct that most drugs are tested, and then approved, at the maximum tolerated dose from Phase I trials. This is to prove efficacy sufficient to get FDA approval. It gives no information on lesser, possibly equally effective dosing. That is, I presume, what you are implying as a “saturation” model. Though I don’t know if the AR kinetics (saturation) with enzalutamide have been worked out. I suspect you are correct as your response shows.
I thought I could work it out. The phase 1 data showed that one dose of 150mg had a halflife of about 5 days - varies with the patient, and that dose reached a maximum in the blood after about 11 days - but we dont know enough about how the concentration in the blood effects the uptake - so I gave up there. Doing a one man test will show what is relevant for me - but others may be different - only do this stuff with the backing of your MO. Depending on the next PSA value in may, I might go down to 80mg to see how the PSA responds. T-A will emphasize that the PSA is not the cancer - but its what we have to work with til we get a new scan.
I am now at the 1/7th of the normal Bicalutamide dose and suspect that I may have to halve it once more. My suspicion arises from the observation that reducing Tamoxifen along with Bicalutamide resulted in breasts getting sensitive, hence had to resume daily dose. PSA next week will show if my suspicion is founded.
Yes. Bicalutamide blocks the AR receptors in the hypothalamus as well as in the PC cells and elsewhere. So the body thinks you have little to no testosterone and causes pituitary to release LH and increase T from the testes. So you have high T even though the Receptors don’t see it. The excess is converted to estrogen, thus stimulating the breast tissue. So the bicalutamide is titrated to cancer/PSA control. (I used 50 mg). And the tamoxifen adjusted to breast control regardless of the bicalutamide dose that works for you. Good approach for as long as it works.
Correct. My T was in the range of 1100 to 1300 before that, due to Avodart. Starting Bicalutamide at normal dose it went over 2500. The lab run the test a second time before releasing the report. Now, with the 50mg/week it has backed off to 1500.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.