I've written a short article introducing a potentially very significant paper - one that should see acknowledgement that not all levothyroxine products are equal.
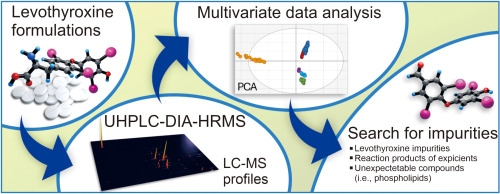
Advancing drug safety and mitigating health concerns: High-resolution mass spectrometry in the levothyroxine case study
Thanks, It's an interesting read, to see how many fillers often indirectly react with the Levothyroxine itself, although certainly not light reading
A couple of points I thought were worth mentioning:
- Why do they use mannitol stearate/mannitol palmitate as a filler when there's reasonable evidence to suggest it can affect intestinal absorption?
- Why do some use citric acid when it's generally considered inappropriate for Levo?
- The oxidative degradation testing is a bit extreme, testing Levo tablets 4-7 years after expiration seems a bit pointless really, when most people will consume them well within date, and the high oxidation results are surely just a good example of why use-by dates are necessary.
thank you for sharing. It mentions citric acid which is in my liquid levothyroxine. With the knowledge that you have please could you suggest is there a liquid levothyroxine that you would say has ‘healthier’ ingredients?
Sorry - no. All UK oral solutions contain some form of citric acid!
I was thinking of exactly this as I read the paper. However, I don't think we can assume that citric acid used in a solid form will have the same effect as in a liquid where (I suspect) it is used to adjust the pH and not for any other reason.
Clearly that needs to be considered in future research.
Citric acid is used in liquid formulations as a stabiliser of the active ingredient and as a buffering agent. It also serves as a preservative, as the slightly acidic pH will prevent bacterial growth.
You would have thought ascorbic acid would work well, it's a a very similar acid, molecularly wise, with the same preservative capabilities, but also has the added benefit of improving levothyroxine absorption.
But obviously I'm not a Chemical Engineer, I'm sure they know what they're doing
Good point, ascorbic acid is often used in food preparation and preservation as well.
I think they use citric acid as it is a much stronger acid than ascorbic acid, and you probably need a lower pH in the liquid formulation to prevent bacterial growth. Just an educated guess though! 😉
And also, I don't think they always know what they're doing! 😂
helvella. you are a dedicated follower and advisor, ipersonally have given up trying to get the correct dose of anything, my own endo once called me in a few years ago as my adrenals were 'off kilter' and ye si have had nasty adrenal problems making me very unwell, but hey a couple of years later he wanted to offload me altogether back to my gp. I disagreed and reminded him of the previous incident, it made no difference, i made a big fuss of not being seen after i had aheart attack a year ago and was then given an appt,
but my tsh was actually in hyper range so i didnt take as much as was on prescription as i was worried it would do more damage,
now i have adjust and trust myself. i have contacted hopsital to find out if i am having any more appts.
all i can say is Helvella, can i make an appointment to see you maybe next week? and thanks for all your imput.👍
thank you Helvella for bringing this paper to our attention. I’m quite convinced that my lupus was induced after many years of levothyroxine use. I also acquired several antibodies one of which was to phospholipids, which I can see from this paper might also be as a consequence of levothyroxine use.
I am astonished to learn that testing is only completed of the pure levothyroxine product rather than the final product. How silly!
Hi Radio2 - I intend to write to the lead researchers (indicated by the small envelope icon next to their names) via email, to congratulate them on their excellent work. I'll mention the possibility of doing similar for Liothyronine too. Anyone can correspond with academic authors, so this is something you could also do 🙂
An issue which has never really made much sense is that different dosages have different effects. We've seen quite a number who have changed from say, two 50 microgram tablets to one 100. Same make. Yet they have gone from being fine to have multiple issues.
It appears unlikely that there is any real change to the active ingredient - nor to any of the excipients. Some tablets are the same size for all dosages - in which case the balance of the excipients to each other will almost certainly be identical. Even while the balance of them to the active ingredient will - obviously - change.
Other makes differ significantly in size. But rarely is a 50 twice the size of a 25, or a 100 twice a 50. Indeed, sometimes the 25 is larger than the 100.
I think this is an issue which is important. And might be affected by things like the ability of oxygen and water vapour to reach the active ingredient deep inside the tablets. As well as when the balances of excipients vary.
But I also hope that this is seen as a first step to the same ideas being applied across all pharmaceutical products.
We have long discussed the issue of generic products versus branded in terms of price more than anything else.
The issues are obviously more complex. Sometimes seeing a cheap generic being better than the brand for some people. But this is a problem when there are multiple generics and it proves difficult to get the specific one which is much better!
If the differences can be identified and understood, we might see the causes of some of the problems being eliminated.
Helvella, I am so grateful for smart people like you!!!
I have encountered changes in formations now four different times with three different T3 brands, each of which initially confused the heck out of me, then led to months of having to retitrate each time to get back to ideal.
I find that I have to retitrate after each brand change, and even with the same brand when they change formulations WITHOUT TELLING ANYBODY!!!
I don't think they ever change the formulation - that is, the things would be listed as the ingredients - without letting us know. But they could change to different suppliers and the differences could be significant.
For example, Merck were very clear there was a new formulation when they launched the new version in France, then around the world.
You are, as ever, absolutely correct helvella ! The absolute formulation cannot change without due notification. However, even the slightest change in things that seems trivial *could* influence the bioavailability of the API.
I had this experience but it could be it was due to one brand purchasing another brand. Dr Reddy’s bought Mayne’s T3 med about a year or two ago and renamed it Dr Reddy’s at the time. I only needed 75mcg of Mayne and the new Dr Reddy’s, but early this year I felt bad on my latest Dr Reddy’s refill and ultimately had to increase my dose to 90 (like i had required on Cytomel and Sigma). I called Dr Reddy’s and they said they had indeed changed their formulation when they started manufacture of their own T3. I suspect now that they were just using up their Mayne supply before they started manufacturing their own with a new formula. But I still think it would have been nice to be notified of the formula change when I refilled my prescription early this year.
What is always a problem is that transferring manufacture can have lots of impacts. For example, changes - even quite modest - to pressure during pressing. And different sources of active ingredient and excipients. Also, it is not impossible that delays in transmission of information from the factory through the FDA can result in mis-matches.
I'd like to know what the Dr Reddy's person meant in admitting a change of formulation. If they really have changed it, then why does it not show?
TBF - I understand your frustrations, but this is a little harsh! There are some excellent, outstanding scientists in India (I have worked with some of them). Agreed - there are also instances of chemical manufacture problems... but this is true of all nations - you only need to look at the FDA warning notices to see this.
So - in this instance, the 'microcrystalline cellulose' might be a case in point (please NOTE: I am *NOT* saying this is what happened, I'm just using this as an example...) Even a small change to the milling of this component might change the behaviour of the T3 within the body. There are chemical factors to consider AND physical factors to consider. Changes in chemical factors, i.e. replacing one excipient with another, constitutes a change and would need to be notified, but using a slightly different crystal size of microcrystalline cellulose is a physical change - and does not constitute a chemical change - so would not, necessarily need to be tested or reported. However, the small active molecule might interact differently with a different crystal size and/or shape, thus influencing its bioavailability.
A materials chemist would recognise this, but a pharmaceutical formulation chemist might not. An analytical chemist would be able to spot the outcome - if a study such as in the paper of helvella's original post is carried out! (With all due respect to pharmaceutical chemists - no insult intended!)
Which seems silly. They've gone to all the bother of identifying it by a ten-character code but don't go the extra step to coding all the variant forms.
Well - precisely! And from a drug formulators POV, they're likely to think they're "much of a muchness"... and most probably cost, availability, and previous trading interactions/tendering process would drive the choice, rather than factors related bioavailability of the API!
Using an inappropriate form of dextrin was partly why Teva was withdrawn from the UK market in 2012. And relocation of manufacturing. And granulation issues.
helvella - thank you so much for posting this paper. You CANNOT believe how happy, and proud, this makes me... so much so that I shed a few tears in reading it! A bit OTT, you may think, but the instrumentation used by the researchers all comes from the company for which I worked for many, many years until very recently.
I can attest that this is a beautifully crafted study, deployed in the most comprehensive of ways. The method development is flawless (IMHO), the data acquisition likewise, the data processing follows state-of-the art unsupervised methodologies, and the results can be considered to be very reliable. [BTW - I have no connections to the universities or researchers involved... this is just my professional opinion, and their work warms my heart!]
Thank you, again, helvella, for a much needed boost to my mood 😊
I'll just throw in a note that at least some specifications for levothyroxine allow it to have up to 1% liothyronine as an impurity/degradation product. Probably not enough to make an obvious impact but just might contribute to the panoply of differences people notice between makes.
Actually, the Liothyronine point was something I spotted on a second re-read of the paper. Made me think it's almost worth keeping some tablets for longer to see if they seem "more effective" - potentially due to having some T3 already present. Feels tempting for poor converters! [PLEASE NOTE: I am NOT advocating taking out of date medication... I'm just "thinking out loud"]
I saw that they found the most T3 in formulations housed within gelatin capsules, which makes me ponder the relative permeability of a gelatin shell versus compacted powder "encapsulation" 🤔
Edited to add: might also be relevant for folks (myself included) who cut tablets to make fractions of masses. The cut surface would not have been expected to be exposed to air and light, so this would change the degradation behaviour... albeit VERY minimally, I should think... but also worth noting.
The amount of thyroid hormone in a levothyroxine or liothyronine tablet is tiny. Something like one thousandth of the tablet.
What would you do to get that tiny an amount to the people who need it? It must be in a form that is visible, and (assuming oral delivery) that can be swallowed. We need to be sure we do swallow it and it doesn't accidentally get stuck between our teeth.
The tablet or capsule needs to disintegrate fully. The active ingredient needs to separate from whatever the tablet or capsule is made of.
While I am very careful to get the same levothyroxine products every time, with most other medicines I really don't take much notice. I've never felt there has been an issue with, for example, a paracetamol tablet due to the excipients used. I suspect many who work in pharmacy don't appreciate the extreme effects of thyroid hormone impurities, degrtadation products, and varying dose delivered?
A significant part of the reason is that if a paracetamol tablet has 20% more, or less, active ingredient, most of us wouldn't notice. But with thyroid hormone - we would. At least, over time or when we change to some which are different in the other direction.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")