Hope everyone is doing fine on your health journey!
I am currently on 25mg T3 (Thybon Henning) and 37.5mg T4 (Euthyrox).
While my symptons are improved, my energy level is stll 7/10 and my weight loss effort is stuck.
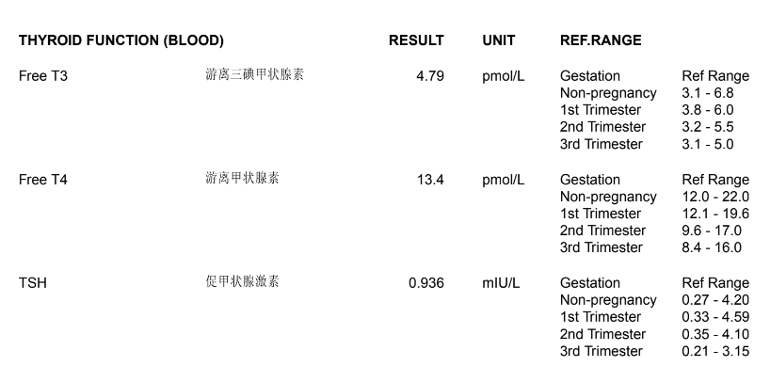
I have recently done my blood test where my free t4 is still low. However, when I increased it to 50mg, I feel very irritable and it worsens my hypothyroidism symptons.
Looking for any advise from people who have had success in tweaking their dosage, please.
Thank you in advance!
Written by
Sofiel
To view profiles and participate in discussions please or .
I take my T3 and T4 medication one shot in the morning. Thanks for your suggestion, maybe I will try splitting my T3 and T4 dosage to see if there're better results.
Which range is appropriate for you - the non pregnancy range?
If increasing T4 to 50mcg doesn't work for you, you could make a smaller increase. I'm on combo meds and when tweaking have found that even a small increase (like 6 or 7mcg when taking around 100mcg daily) can make a big difference and this can be achieved by working out over a week how to alternate doses to achieve the desired exact dose.
Obviously see if splitting dose, as SlowDragon has suggested, works before doing anything else.
How do you tell what is the optimal combination of the medication for you? Would you also be able to share how you alternate the doses weekly? Thank you!
How do you tell what is the optimal combination of the medication for you?
You will know by how you feel, ask yourself do you feel well, could you feel better, have all your symptoms abated, etc. It can take a long time and much tweaking of the individual hormones to find the perfect combination, much patience and time is needed.
Would you also be able to share how you alternate the doses weekly?
You don't alternate doses weekly, you work out how much per week you need then alternate the dose during the week.
For example, I was taking 112.5mcg Levo daily. My FT4 was a bit too high and I wanted to lower my dose slightly to bring it down a bit and I wanted to average 107mcg daily. I only have 100mcg and 50mcg tablets but I have a pill cutter so I can cut the 50mcg tablets.
107 x 7 = 749mcg per week (so let's say 750mcg)
So I would need 7 days at 100mcg to give the 700 and need to find a way to split the 50mcg over a week. I can only split the 50mcg into quarters, ie 12.5mcg, so to even things out as much as possible I need to add 1/4 of a 50mcg tablet to a 100mcg tablet on 4 days. This is how I did it
Monday - 112.5mcg
Tuesday - 100mcg
Wednesday - 112.5mcg
Thursday - 100mcg
Friday - 112.5mcg
Saturday - 100mcg
Sunday - 112.5mcg
This adds up to 750mcg per week which gives an average of 107mcg per day.
You might be right! I felt stressed & edgy and had difficulty in controlling my temper when I raised it. It also triggered my cravings for savoury carbs i.e. pizza, potato chips.
Ooof yes. That sounds very cortisol. Hypoglycemia and edgy are cortisol 🚩🚩 for me.
I am not a medical professional. I have just collated helpful information available on adrenals found in different, reputable thyroid help books.
Adrenals do not get enough recognition for their essential role in the effective metabolism of thyroid medication. For some people taking thyroid medication is enough to get adrenals working again, for others it isn’t.
If you are having problems raising/tolerating/having no benefit from/feeling worse from your thyroid meds consider cortisol.
Low cortisol symptoms (these are not exclusive to low cortisol):
Negative or no response to thyroid medication
Chest pains
Nausea
Fatigue
Insomnia
Waking through the night
Anxiety
Depression
Abdominal fat
Poor stress tolerance
Weight gain or loss
Tinnitus
Low blood pressure
Dizziness on standing
Sensitivity to light
Palpitations
Thumping heart beat
Menstrual irregularities
Hypoglycemia
High or low appetite
Headaches / head pressure
Pigmentation / melasma
Burn in the sun instead of tan
"At least 50% of hypothyroid patients may have an adrenal problem and without discovering and treating that problem you will be unable to benefit from thyroid treatment." (Stop The Thyroid Madness, Janie Bowthorpe)
"Low cortisol causes T3 to work less effectively within the cells. This is because T3 and cortisol are partners within our cells. High cortisol also causes problems and can reduce the effectiveness of T3 within the cells, hence thyroid patients with high cortisol often complain of feeling hypothyroid even when they appear to have reasonable or low FT3 levels. When patients try to raise T3 levels in the presence of low cortisol, they may find that the body compensates for low cortisol by producing more adrenaline. This can cause anxiety, rapid heart rate, the feeling of heart palpitations etc. This is usually the adrenaline response rather than a direct issue with the T3. Very often, it is the low cortisol that is at the root." (Paul Robinson website)
"Whatever you may be told, adrenal insufficiency in thyroid disorders is very common indeed and should always be considered at the onset of treatment. Failure to respond to thyroid supplementation, or actually feeling less well, is likely more often than not to involve the low adrenal reserve syndrome." (Peatfield “how to look after your thyroid”)
"If, upon starting NDT [or T3], you experience symptoms, including anxiety, insomnia, shakiness, sweating, dizziness, feeling spaced out it's a strong sign that you may need adrenal support." (Tpauk website)
Adrenal testing: 4 point saliva test from Regenerus Labs is good if you suspect moderately low cortisol.
If you think you have a more profound cortisol issue then you need to ask your GP for -
SYNACTHEN
ALDOSTERONE
RENIN
ELECTROLYES
ADRENAL ANTIBODIES
Blood tests are inferior to saliva tests because bloods show what is total, saliva shows free and therefore available. But bloods are still valuable and a very important step in ruling out anything more serious than adrenal fatigue.
Interpreting saliva results: Morning sample must be the number at the top of the range, midday must be 75% through the range, afternoon must be 50% through range and evening must be below the top part of the range. If anything comes up lower than this, then this indicates low cortisol. (If cortisol is high then this can be lowered through Phosphorylated Serine)
Interpreting blood results:
A 9am morning cortisol results needs to be in the top 1/4 of the range at least, anything less can be indicative of adrenal insufficiency and needs to be followed up by your GP.
A synacthen test is where the adrenals are artificially stimulated by ACTH (the signal that comes from the pituitary to the adrenals) to see what adrenal hormone you can produce. This test will show you whether you have a primary (with the adrenals) adrenal issue, or a secondary (with the pituitary - therefore the signal that is sent to the adrenals and not the adrenals themselves) adrenal issue. If ACTH is low this is indicative of a pituitary issue (secondary adrenal issue), this can often be rectified by incorporating T3 in your treatment as the pituitary is particularly T3 reliant. If your response to the synacthen is below 420 and/or does not double from the previous result then we can assume a primary adrenal issue.
Aldosterone is a steroid created in a different part of the adrenal cortex. If this comes up low and renin high in conjunction with low sodium then this is further suggestive of a primary adrenal issue (so the adrenals themselves).
Low Cortisol Treatment (after testing):
If you fail a synacthen test this is indicative of adrenal insufficiency and steroid replacement of hydrocortisone will be warranted. This is usually in the realm of 20mg-40mg a day, if Addison’s antibodies are present this replacement will be for life. Sometimes Fludrocortisone is also needed, this is usually around 0.1mg. If you are placed on Fludrocortisone you will need to watch potassium levels, and ask your doctor for extended release potassium if your potassium drops too low. It is also important to invest in high quality salt and liberally use it.
If you have low cortisol and low ACTH but pass the synacthen test this is indicative of a secondary adrenal issue - an issue with the pituitary. This can often be rectified by T3, it is worth trying Paul Robinson’s CT3M for this.
For mildly low cortisol -
According to STTM:
Adrenal Cortex Extract (not whole adrenal gland): On waking 150mg, 100mg at noon, 50mg afternoon, 50mg evening. After 5 days on those doses you can do DATS (Daily Average Temperatures) - Measure BBT 3 times; 3 hrs after waking, 3 hrs after that, 3 hrs after that and add them up to make an average, do this 5 days in a row avoiding ovulation & menstruation. If there is more than 0.2 degrees fluctuation between the temps then Adrenal Cortex Extract needs to be increased. Increase Adrenal Cortex Extract until DATs become stable. If DATs do not ever become stable then Hydrocortisone may be needed. STTM states 25mg/day is a starting dose, broken down as: 10mg on waking, 7.5mg at noon, 5.5mg in afternoon, 2mg before bed. If DATs still won't stabilise then this could indicate an Aldosterone issue.
According to Peatfield:
Adrenal Cortex Extract: Anywhere from 150mg to 600mg in the morning and nothing after midday. He also recommends 20mg of Hydrocortisone for those who are not improved by Adrenal Cortex Extract.
According to Paul Robinson:
Research CT3M (Nb. Many do not find this effective).
Nb. Initially cortisol presence can increase thyroid hormone uptake so much that you may feel over stimulated/strange. Some advise to lower thyroid hormone dosing to let thyroid hormones run down a few days before starting ACE to avoid this.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.