I’m new to the group (finally joined, which my mum will be relieved to see!) and hoping for some advice about how I can move forward after having 3 miscarriages in just over a year.
I conceived my little boy in 2019 - 6 months after being diagnosed with Hashimoto’s. I was prescribed 50mcg of levothyroxine per day and this was increased slightly during my pregnancy, but only at the end as far as I can recall. I’ve since only been taking 75mcg daily, and didn’t have my dose increased during subsequent pregnancies. I can’t seem to carry the pregnancy past 10 weeks and I’m now only seeing the light that I perhaps should’ve been increasing my dose in those first few crucial weeks.
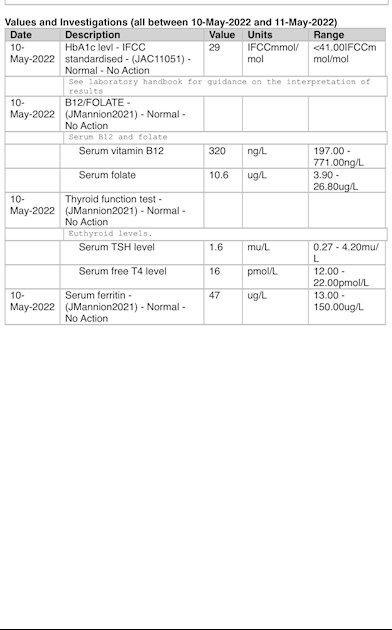
I’ve attached a photo of my most recent blood test results that were done through the NHS. The second photo shows my results from Medichecks which were carried out approximately 2 weeks before the NHS tests. I opted for tests to be done through Medichecks as I was so angry that I’d not had a single blood test done from the start to the end of my most recent pregnancy. In hindsight, I wish I’d been more proactive about my thyroid condition rather than fixating on progesterone as the solution when in fact it wasn’t, sadly.
Does anyone have any insight into reasons behind recurrent miscarriages when diagnosed with hashimotos? I suppose I’m just looking for answers whilst waiting to see a specialist, as it looks like there are no appointments available in the near future! Thanks in advance.
Amy
Written by
MadeinCayman
To view profiles and participate in discussions please or .
Eating iron rich foods like liver or liver pate once a week plus other red meat, pumpkin seeds and dark chocolate, plus daily orange juice or other vitamin C rich drink can help improve iron absorption
This is interesting because I have noticed that many patients with Hashimoto’s disease and hypothyroidism, start to feel worse when their ferritin drops below 80 and usually there is hair loss when it drops below 50.
Thyroid disease is as much about optimising vitamins as thyroid hormones
I eat red meat and have a really good diet generally - lots of variety - but I need to make sure it’s consistent. I was taking prenatal vitamins but I’ve stopped now, although I should start taking them again in case. I’ve lost so much hair lately. Thank you
Thorne Basic B or Jarrow B Right are recommended options that contains folate, but both are large capsules. (You can tip powder out if can’t swallow capsule)
But wether you should take this or just a folate before TTC you will need to read and decide
IMPORTANT......If you are taking vitamin B complex, or any supplements containing biotin, remember to stop these 7 days before ALL BLOOD TESTS , as biotin can falsely affect test results
With serum B12 result below 500, (Or active B12 below 70) you might want to be taking a B12 supplement as well as a B Complex (to balance all the B vitamins) initially for first 2-4 months.
once your serum B12 is over 500 (or Active B12 level has reached 70), stop the B12 and just carry on with the B Complex.
Thank you so much for your advice and guidance. I really appreciate it. I couldn’t post the results from medichecks (done 2 weeks before NHS tests and they include FT3 too) but here they are. I had bloods taken in the morning but not before 9am. I’ll ask to be retested soon and will follow your advice, thanks. I didn’t take meds on the morning of the tests. I hadn’t realised the difficulty hashimotos patients have with processing folic acid. This is an interesting read. I don’t know why I had no problems conceiving my son but have since had so many issues. I was actually prescribed a higher dose of folic acid during my most recent pregnancy alongside progesterone. I’ve had a lot of hair loss since the 3rd miscarriage (ended at 10 weeks last month).
Thank you for your time and for sharing your knowledge. I’m still learning about the condition I have.
Just for future reference, if you click on the icon, top right of your Medichecks report, you get the option of downloading the printable PDF, that will give your results in one page.
I’m awaiting the results of the vitamin D test that was done through the NHS. I had the miscarriage around the 8th of April but didn’t have blood tests done until the end of April through Medichecks, and 10 days ago through the NHS. Thank you everyone for all your assistance.
I meant to add earlier that I’ve never had a coeliac test done but I’ll look into it, thanks.
I also meant to add to my original post that I had a consultation with a miscarriage specialist at Spire 2 weeks ago (half an hour conversation and review of my Medichecks blood tests) who advised me to increase my dose by 25mcg. I followed his advice but didn’t think for a minute that the impact would be detected in the NHS blood tests so soon after the increase in dose (just a few days). Is this possible? There seems to be a real difference between each set of results.
Initially Ft4 will shoot up …..because the body’s not been use to the increase in levothyroxine
Then slowly over 2-4 months your body gets use to having the increase…..your overall metabolism improves…..Ft4 begins to drop…because your using more ……by then likely ready for next dose increase
When on levothyroxine and TTC …..dose levothyroxine is normally increased immediately conception is confirmed
I was prescribed 50mcg of levothyroxine per day and this was increased slightly during my pregnancy, but only at the end as far as I can recall.
I'm sorry to say, but your doctor was negligent in leaving you on such a low dose of thyroid hormone during pregnancy. When people get pregnant the fetus doesn't immediately sprout a thyroid, so it needs thyroid hormone from the mother. Increasing thyroid hormone dose should be done as early as possible during the pregnancy, not right at the very end!
Low thyroid hormone levels will reduce your chances of conceiving and will also increase your risk of miscarrying.
For info on thyroid development in the fetus see this link :
In the first trimester, the developing fetus is initially dependent upon maternal thyroid hormone crossing the placental barrier.[1] Around week 16 (GA week 18) the fetal thyroid becomes active enough to support the fetal requirements for neural development.
Maternal thyroid hormone - required for early stages of brain development (Maternal Thyroid recent studies show both high and low thyroid hormone impact)
Fetal functions from week 10 - required for neural development, stimulates metabolism (protein, carbohydrate, lipid), reduced/absence = cretinism (see abnormalities)
Maternal thyroid function also changes in early pregnancy, through pituitary changes, resulting in thyroid stimulating hormone (TSH) levels decreasing during the transition from pre-pregnancy to early pregnancy.[2] This change in TSH was less predictable in women with thyroid antibodies. Generally maternal TSH and free T4 are maintained within the same range as those in nonpregnant women.
Thank you for the information and for taking the time to respond. I completely agree and I am so angry at such neglect over the years. I need to self-advocate from now on and push for further testing and advice.
I’m so sorry to hear what has happened. I too had miscarriages but I went on to have 2 healthy babies in the end. I have Hashimoto’s and now have an excellent private doctor who prescribes and monitors my medication. Thyroid UK do have a list of private doctors in case you feel it’s worth going down that route. All the best to you for the future.
Sorry to hear you’ve been through this too - I’m so glad that you went on to have successful pregnancies. I’d really love to give my son a brother or sister but I know how blessed I am with my current situation.
Even if we frequently don’t start on full replacement dose, most people need to increase levothyroxine dose slowly upwards in 25mcg steps (retesting 6-8 weeks after each increase) until eventually on, or near full replacement dose
Consider starting levothyroxine at a dosage of 1.6 micrograms per kilogram of body weight per day (rounded to the nearest 25 micrograms) for adults under 65 with primary hypothyroidism and no history of cardiovascular disease.
Traditionally we have tended to start patients on a low dose of levothyroxine and titrate it up over a period of months. RCT evidence suggests that for the majority of patients this is not necessary and may waste resources.
For patients aged >60y or with ischaemic heart disease, start levothyroxine at 25–50μg daily and titrate up every 3 to 6 weeks as tolerated.
For ALL other patients start at full replacement dose. For most this will equate to 1.6 μg/kg/day (approximately 100μg for a 60kg woman and 125μg for a 75kg man).
If you are starting treatment for subclinical hypothyroidism, this article advises starting at a dose close to the full treatment dose on the basis that it is difficult to assess symptom response unless a therapeutic dose has been trialled.
Welcome to our forum and sorry to hear about your miscarriages.
Both Vit B12 and folate need raising, and you need to get an FT3 test to evaluate a comprehensive level of thyroid hormone, ferritin is quite low and an iron panel with give you a better view of how iron is working. Have you had Vit D levels tested?
You appear to have been left under-medicated. Adequate levels of thyroid hormone are not only essential for pregnancy retention, healthy fetal development and to support your own expanded metabolic needs but also to reduce thyroid activity and help keep thyroid antibodies low in the case of Hashimotos.
There is research and literature correlating elevated TPO antibodies to adverse pregnancy outcomes. Are you managing thyroid antibody levels with for example a g/f diet and supplementing selenium?. For information on how Hashi can impact conception & pregnancies a good book is ‘Your Healthy Pregnancy With Thyroid Disease" by Dana Trentini and Mary Shomon.
I appreciate your response and help. I’ve included my vitamin d results above but I don’t trust that they are ‘normal’. I’ll take a look at your recommendations, thank you. FT3 was tested by Medichecks and was 3.75.
My daughter’s Gp reduced her thyroxine from 175mcg a day to 150mcg a day and she had a miscarriage. Upped it back to 175mcg (which she was on all the way through her first pregnancy) and she went full term. You are on a very low dose so maybe you do need a higher dose. Your FT4 is quite low in the range and possibly needs increasing.
Thanks to you all for taking the time to respond and helping me understand my diagnosis that bit more. I’ve managed to book an appointment on Monday with a consultant at a local hospital (a cancellation appointment came up today - they’re like gold dust as there’s a huge backlog & I honestly thought I’d be waiting months) so I’ll post the next steps of my journey for those who may be interested. I have lots of questions for the consultant!
I’m so sorry you’ve been through this MadeinCayman. Like others here, I’m wondering about your vitamin B12 levels as low vitamin B12 is often implicated in failure to conceive and other problems, and is often linked with thyroid disease.
This is one of the best reviews of one of the best books on B12 deficiency I’ve read. Sally Pacholok has also written a later book for mothers and babies and the WestonPrice website has v. good information on nutrition generally for this category.
Thank you so much for the information and advice. I’m hoping to be monitored much more closely now that I am under a consultant/fertility specialist. I received a call from the hospital on Friday offering me a cancellation appointment on Monday which I happily took and attended 😊. My hashimotos will be monitored and I also had blood tests for APS to see if there’s a problem with blood clotting etc. I need to focus on B12 too however.
Without reference ranges we can't tell whether your Free T4 is high in range or over the range.
Also, you really need a Free T3 test as well, but the NHS very rarely tests it. You can get tested with a finger-prick blood sample from an NHS lab which does private testing:
Okay, so the TSH and Free T4 ranges are the standard ones.
Your TSH is much better than some of the earlier results you've quoted. Some of us need it to be lower still to feel well, but it may take a while to tell whether you will feel well or not.
Your Free T4 being high in range is also an improvement.
You could find that the drop in TSH and the increase in Free T4 don't last long as your body adjusts, so there is no guarantee that you are on the right dose yet. It could be slightly too high or slightly too low. It's impossible to guess.
And the thing you really need to know is your Free T3, preferably after you've been on your current dose for 6 - 8 weeks. Low Free T3 will give you hypothyroid symptoms, and high Free T3 will give you hyperthyroid symptoms. But high Free T3 won't make you hyperthyroid. Since you are hypothyroid, your thyroid can't regenerate and start producing too much thyroid hormones - but you can be over-medicated.
It is also important to get the basic nutrients optimised. But dealing with these can sometimes take ages, depending on how well you absorb nutrients. Some nutrients will improve faster than others. Iron tends to be very slow, for example.
Thanks again for taking the time to respond. I really am still learning about my condition/the medication/supplements etc as I hadn’t realised that a higher FT4 would be a good thing. There’s so much information to process and I know I’ll need to test as often as possible to make sure I’m on the correct dose.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.