My daughter had her thyroid checked straight after Covid. She was being monitored after a very brief period (less than 2 weeks) of hyper last year. Asymptomatic, no medication. No ranges provided this time, but looking at ranges from previous tests it looks like free T4 is within range (21.8) free T3 high, TSH low (undetectable) antibodies high (TSH receptor IGG AB 2.77) Could this be simply due to the recent Covid infection? They suspect Graves and want to put her on Carbimazole. GP knows about the Covid, but don't think that the hospital who advised the GP to describe the medication knows.
Can Covid affect thyroid levels? : My daughter... - Thyroid UK
Can Covid affect thyroid levels?
Written by

bgar11
To view profiles and participate in discussions please or .
Read more about...
50 Replies
•
yes according to some initial reports, it seems it can , but i don't know if you can blame it for the raised TRab (that indicate graves disease) ? what was the level of TRab last time ? However if fT4 is currently in range and fT3 is only slightly over the range , i think it's bit premature to be using anti thyroid medication unless she has symptoms of hyperthyroidism that are causing problems.
Personally i'd want to watch and wait .. especially in light of the possibility that covid could have had an effect.
Thanks for your reply. I'd also read info on connections between Covid and thyroid results. Personally, as there are no symptoms, I'd retest (although now she's just had her first dose of Pfizer so wondering if that could also affect results). Her last IGG AB was at the beg of Dec and was a bit higher than this one (3.51 at the time 2.77 now). It was done because of her first and to date only episode of hyperthyroidism symptoms, which only lasted a few days. By the following test, on 15/12, both T3 and T4 were back within range naturally. TSH was still low. Values were progressively improving in following follow-up tests until this post Covid one on 30/6 (she had only recovered from Covid a few days before the test).
if TRab have lowered from previously ,, i'd think that is even more reason to 'watch and wait' , rather than take carbimazole.. as nobody really knows what, if any effects covid /any jab could have on graves/thyroid ,...i'd wait and see. and test again later. if she had fT4 /3 several times over the range's it would be different , and would need dealing with, but currently fT3 only looks to be slightly raised. (what is the range on that fT3 test ?)
If symptoms are only occasional , they could use other medications rather than antithyroid drugs .. i forget what , but they do sometimes give other things just to help with symptoms.
I would have though that taking antithyroid drugs when fT4 is in range and fT3 is only slightly raised would just lead to fT4 /3 going too low.
Thanks for the advice. Yes values were only high for a few days at the end of Nov/beg of Dec last year and again now (but only T3 now ). No ranges provided this time, but the ones in previous tests were free T 3 3.1-6.8. and free T4 12-22. Antibodies IGG AB 0-2. No symptoms this time. The problem is convincing the GP to retest. She wants to retest after starting Carbimazole because I think that she's sticking to the instructions from the hospital (but the hospital doesn't know about Covid). I think that she should inform them of this, but that's what she's not doing. After pointing out that connections between the two are listed online, she's had a quick look and said that it's possible, but not proven, etc. (I think that expecting several proven studies is a bit much considering how recent Covid is. Conducting research studies takes time!!!)Are we allowed to mention hospitals and names of endos on here?
Are we allowed to mention hospitals and names of endos on here?I don't think so.. except to write a post asking for private messages if any one has any experience of them.
surely if daughter say's "no thanks" to the carbimazole for the time being.....then GP will have no choice but to retest thyroid bloods at some point ?
I think the covid? issue is not the point .. if she has no symptoms and fT3 is only slightly over -range then why would she want to take the carbimazole anyway... she doesn't have to if she doesn't want to.... so in that sense it doesn't matter if covid has had an effect or not.
SlowDragonAdministrator
Test TSH, Ft4 and ft3 together early morning
Has she had TSI or Trab antibodies tested for Graves’ disease
Or TPO and TG antibodies for Hashimoto’s.
She also needs Vitamin D, folate, ferritin and B12 tested too
Thanks for the reply. Tests were done early morning. The antibodies test was IGG AB. Unfortunately Vitamin D and B12 were not checked this time although we were initially told they would be
Test results
No range on results
Red blood cell width highlighted as abnormal
healthline.com/health/rdw-b...
No folate, ferritin, B12, vitamin D or thyroid antibodies
Yes, I used the ranges from the previous tests as this time the ranges were not included
You can’t assume they are same, might be different lab
" The antibodies test was IGG AB."
Just to clarify... from original post you wrote:
"antibodies high (TSH receptor IGG AB 2.77) "
Graves antibodies are called 'Thyroid stimulating hormone Receptor antibodies '
It can be written in various ways ,including TRab or T(sh )Rab or TSH receptor ab.
I'm not used to seeing 'IGG' as part of how it's written., but i'm pretty sure the result you put above is a TRab (Graves antibody) result,
I think it will be confusing people if you call it IGG
IGG is not a specific antibody:
Immunoglobulin G
Immunoglobulin G (IgG) is a type of antibody. Representing approximately 75% of serum antibodies in humans, IgG is the most common type of antibody found in blood circulation.[1] IgG molecules are created and released by plasma B cells. Each IgG antibody has two paratopes.
en.wikipedia.org/wiki/Immun...
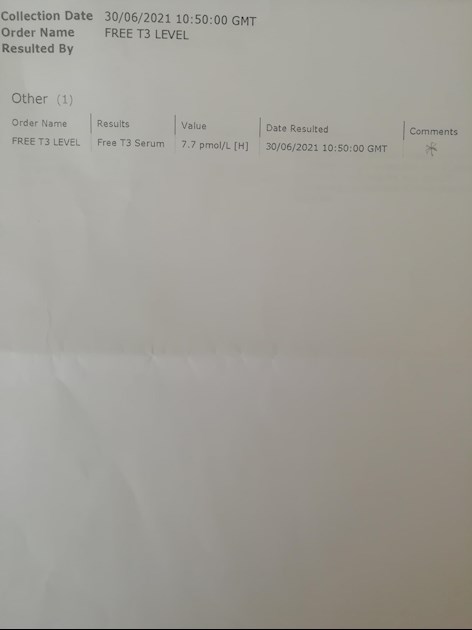
Thanks. I'm attaching a picture of the result to clarify which test she's had done.
Antibodies test
Thanks,, so lots of different antibody tests could say IGG on them ?
Yes -lots and lots of them. Some 75% of antibodies are Immunoglobulin G.
This is the one they have done
Antibodies test
yes .. clearly says TSH Receptor antibodies .. that is a TRab (graves )test. I think you can ignore the Igg bit .. i think it's just 'lab speak'
There are, though, three types of TSH Receptor antibody - stimulating, blocking and neutral. The result, as presented by the lab, is consistent with, but not absolutely diagnostic for, Graves.
TSH RECEPTOR ANTIBODIES: RELEVANCE & UTILITY
George J Kahaly, Tanja Diana, Paul D Olivo
• PMID: 32022598
• DOI: 10.4158/EP-2019-0363
Abstract
Objective: Antibodies (Abs) to the thyrotropin (TSH) receptor (TSH-R) play an important role in the pathogenesis of autoimmune thyroid disease (AITD). We define the complex terminology that has arisen to describe TSH-R-Abs, review the mechanisms of action of the various types of TSH-R-Abs, and discuss significant advances that have been made in the development of clinically useful TSH-RAb assays. Methods: Literature review and discussion. Results: TSH-R-Abs may mimic or block the action of TSH or be functionally neutral. Stimulating TSH-R-Abs are specific biomarkers for Graves disease (GD) and responsible for many of its clinical manifestations. TSH-R-Abs may also be found in patients with Hashimoto thyroiditis in whom they may contribute to the hypothyroidism of the disease. Measurement of TSH-R-Abs in general, and functional Abs in particular, is recommended for the rapid diagnosis of GD, differential diagnosis and management of patients with AITD, especially during pregnancy, and in AITD patients with extrathyroidal manifestations such as orbitopathy. Measurement of TSH-R-Abs can be done with either immunoassays that detect specific binding of Abs to the TSH-R or cell-based bioassays that also provide information on their functional activity and potency. Application of molecular cloning techniques has led to significant advances in methodology that have enabled the development of clinically useful bioassays. When ordering TSH-R-Ab, clinicians should be aware of the different tests available and how to interpret results based on which assay is performed. The availability of an international standard and continued improvement in bioassays will help promote their routine performance by clinical laboratories and provide the most clinically useful TSH-R-Ab results. Conclusion: Measurement of TSH-R-Abs in general, and functional (especially stimulating) Abs in particular, is recommended for the rapid diagnosis, differential diagnosis, and management of patients with Graves hyperthyroidism, related thyroid eye disease, during pregnancy, as well as in Hashimoto thyroiditis patients with extra-thyroidal manifestations and/or thyroid-binding inhibiting immunoglobulin positivity. Abbreviations: Ab = antibody; AITD = autoimmune thyroid disease; ATD = antithyroid drug; cAMP = cyclic adenosine 3',5'-monophosphate; ELISA = enzyme-linked immunosorbent assay; GD = Graves disease; GO = Graves orbitopathy; HT = Hashimoto thyroiditis; MAb = monoclonal antibody; TBAb = thyrotropin receptor blocking antibody; TBII = thyroid-binding inhibiting immunoglobulin; TSAb = thyrotropin receptor-stimulating antibody; TSB-Ab or TRBAb = thyrotropin receptor-stimulating blocking antibody; TSH = thyrotropin; TSH-R = thyrotropin receptor.
pubmed.ncbi.nlm.nih.gov/320...
Wow! Thanks. So we are still not sure it's actually Graves if I understand correctly. She had an ultrasound in April and they said that there was no damage. They said it looked like a thyroid which had been inflamed but was recovering (blood results were consistent with that at the time. T3 and T4 in range. TSH improving. Antibodies were not done then)
Thanks
SlowDragonAdministrator
I would suggest you get full thyroid and vitamins tested via GP before agreeing to Carbimazole
GP should retest TSI or TrAb antibodies
Thanks for the advice. The IGG AB were tested. I'm attaching a picture. Yes, persuading GP to test the rest is really difficult
Test results
Really? That's what they think is indicating Graves. Why don't they do one of the tests that you have mentioned then? Are they more expensive?
Sorry yes you’re correct
Test confirms Graves’ disease
Thanks. Is it definetely Graves? Would you start taking Carbimazole now even if no symptoms and only T3 is above range? Antibodies have lowered in comparison to last year 2.77 now, while 3.57 at the beginning of Dec, so better now. No meds so far. All the T4/T3 tests between Dec and now were in range (only TSH low). Now T3 is raisedAccording to ranges used in previous tests T4 is still in range (the upper value in previous ranges is listed as 22).
Free T4
Hopefully other Graves patients might comment
Eg PurpleNails
i think it is a TRab result, ,but report say's IGG in name as well
PurpleNailsAdministrator
Until levels are continuously rising or very high you could chose to delay commencement of carbimazole. Especially if no symptoms are present.
I was diagnosed hyper with similar level of FT3. I did have symptoms but my levels had risen so gradually I hadn’t noticed at the time. Does your daughter have a fit bit or way to monitor heart rate?
An earlier post said she had been on propranolol, has this been stopped?
Try to find out what sort of dose the doctor will be recommending & how frequently they intend to retest levels and adjust medication. This could help inform the decision.
If the dose suggested is high with very infrequent or spaced out monitoring, then I’d resist longer.
Carbimazole will lower production of new thyroid hormone. Up go 60mg starting dose can be given to those with very high levels. Lower doses are given to levels not as high. I started on 20mg, with adjustments to 10mg, then 15mg, then 10, 15 different days. Currently 5mg, 10mg alternating days. 5 mg is usually a maintenance dose.
As your daughter does have positive TRab maybe there is a case for low dose to see if it helps settles & stabilise levels.
Thanks. Propano was only taken for a few days in Dec when she had symptoms. No symptoms since then. No medication. T3 and T4 back in range by mid Dec and again when tested in Feb and Apr. Only raised on 30th June, but test was straight after Covid.TSH was still low but improving. Gone back to undetectable this time, I. e end of June.
Antibodies are lower this time than they were in Dec, but still above range. Ultrasound in April showing no damage to thyroid, no nodules, etc. 'A thyroid that is recovering after an inflamation' was what the person doing the scan said.
Would an oxymeter which also measures the pulse do for the heart rate?
I will know about dosage next week. I cannot deal with the GP directly as my daughter is 19, so not a minor.
I think that she said she's going to monitor her closely, but promises don't always materialise, plus once my daughter is back at uni in Sept, she will be under the care of two different GPs so there might be communication issues too.
Thanks for all the info on dosage. I really appreciate it. Is Carbimazole taken just to keep levels within range (and control symptoms) or does it also help with the underlying cause, if that is Graves after all? Is there a definite test to determine if the cause is Graves?
Usually positive TRab or TSI is taken as evidence of Graves.
Were any other antibodies tested?
It’s good she has had a ultrasound scan as this would identify any nodules and areas of damage eg damage left by autoimmune attacks, thyroiditis. Do you have a copy of the specialist report? Usually a specialist will review the images and report back to referring physician. Always obtain copy of it as might (not always) give more information than what was said verbally during the appointment. Contact the department direct & ask for a copy.
I had negative TSI result but ultrasound showed a large nodule, so I had a specialist thyroid uptake scan. This shows the entire thyroid function. The patterns are distinctive and clearly shows normal function in comparison to over / under active areas of the thyroid. (Which an ultrasound can’t do conclusively).
Antibodies wax & wane and medics don’t know how & why they vary or how to treat them directly. They are used for diagnosis and often not ever repeated. Although it is known that low Trab levels indicate a better the chance of remission when stopping carbimazole. Retesting is not routinely done.
I have heard or doctors advising patients to start carbimazole when TSH is low even if levels are still in range as it “protects”. In other words they are implying it has an action on the underlying cause but I’ve never seen any research actually supporting this. Carbimazole known mechanism is inhibitory on hormone production and not known to directly impact the immune system.
A pulse oximeter would give a current reading so taken several times a day is better than nothing. A tracker with continuous reading and resting heart rate would be better. My pulse is quite well correlated to thyroid levels so useful long term.
Thanks for all this info and advice. I don't have a copy of the ultrasound report, but we could request it, as you suggested.No other antibodies were tested this time. The same antibodies were tested at the beginning of zdecembrr last here and they were a bit higher than now.
Thyroid peroxidase IGG AB were tested in Feb and they were raised, but the report said that it was a weak positive which didn't necessarily indicate thyroid disease
So would a raised pulse several times a day be indicative of hyperthyroidism? How high would it have to be to be indicative of this?
Do you have Graves? If so, what do you do to control it? Any dietary/lifestyle measures?
There can be an overlap with antibodies with TPO & TGab having highest elevations with Thyroiditis and TRab and TSI having the highest elevations with Graves. Antibodies can appear in either condition and it’s also possible to have both conditions.
I have a diagnosis of a large solitary hyper functioning or hot / toxic nodule. It causes continuous hyper which isn’t autoimmune & doesn’t have the possibility to resolve which is the goal with Graves.
When I was diagnosed my TSH was undetectable, FT4 borderline high & FT3 almost 2x the normal level. I had gained a lot of weight despite being mildly hyper. My theory is this was due to an out of control appetite, zero energy & motivation which developed so gradually I hadn't notice. I also had headaches & my once nice nails were lifting off their beds.
I had resting heart rate averaging 80bpm & an ecg reading of 102 after a short walk. The GP advised me contact the endocrinologist myself that day to see what they wanted to do, so he couldn’t have been that concerned. These days my resting rate is around 65.
I’ve now been taking carbimazole 2 and half years. Starting dose 20mg currently 7.5mg per day.
Within a year of starting medication I was also diagnosed with type 2 diabetes. I think the high thyroid levels contributed to worsening it. I lost weight with a low carb diet & increase in activity, this helped the thyroid levels as well as the blood sugar levels. Many recommend gluten free with Graves but it’s no something I’ve attempted.
Graves more often presents as levels spiking sky high suddenly. Whereas with hot nodules like mine the levels rose very slowly. I was keen to find out what my levels were normally so tracked down results from a blood test taken 4 and half years before my diagnosis. I was rather shocked to learn that although my antibodies and FT4 was Normal. The TSH had been undetectable and FT3 was slightly over range. I was pretty riled I hadn’t been informed and no rechecks during the entire time.
Not knowing did save me those years from starting carbimazole. So maybe it did work out for the better? I do sometimes have concerns about what slightly elevated thyroid levels for 4 plus years might means long term. Im quite sure having a suppressed TSH for years is the reason my TSH has never recovered and still remains under-range even though my level are euthyroid.
I don’t know when it would have been the best time to start medication even knowing what I learnt now and knowing that my levels would go on to rise continuously. It wasn’t in my control and it must be difficult to judge what’s best for your daughter. Theres no easy answer.
Keep monitoring, consider a low dose of carbimazole if levels remain high & follow by your instincts.
Sorry to hear about your nodule and that they didn't inform you of your elevated levels for years. In my opinion copies of tests, with highlighted out of range values, should be sent to patients automatically, without having to be requested. Al least now you are on a low dose and euthyroid.
I've read in another thread that sometimes TSH can take a very long time to get back in range even after the other values are back to normal. In this person' s case it took two years. Hopefully yours will eventually go back within range too.
I will tell my daughter about taking her resting pulse several times a day to see if it is elevated and so get an idea of her thyroid levels.
I seem to understand that the contrast test is the only one which can determine clearly the cause of the hyperthyroidism (Graves, thyroiditis, etc.)
Thanks so much for all the info and advice. Really valuable.
Recommend wearing a Fitbit or equivalent to monitor resting heart rate and activity levels
You can print out weekly summaries too for medics
Thanks for the tip. Would the GP provide this? I assume not and that I would have to purchase it. Would I be looking for sudden rises or for a steady high rate? Is high 80 or above?
You would need to buy your own Fitbit
Wearing at night especially useful to see true resting heart rate
When hypothyroid many of us have resting heart rate below 50
Hyperthyroid obviously looking for high resting heart rate
Thanks
Covid and the covid jab are both excititory so things can go haywire on all fronts if it was my daughter I would want to wait for things to settle down , so I agree with tattybogle
Many people have reported flare ups from covid and the jab - this is to be expected from the jab bc it stimulates the immune system
Thanks for this. I thought the same, given that it stimulates an immune response. It'd be interesting to know what endos think/say about this, but communicating dire tly with the endo is impossible outside app times. My daughter is going to discuss this issue with the GP again when she sees her on 9th Aug. She doesn't want to start on Carbimazole now. She's asymptomatic. I'm worried that the med can give her hypo symptoms and make her feel worse
does a positive TshRab always indicate graves ? .. in this case (due to the TSh being low and fT3 being raised ) almost certainly "yes." because this is what effect the 'stimulating' type of TshRab have ... they mimic the action of TSH . prompting the thyroid to make more T4/3 and increasing the conversion of T4 to T3, and because the pituitary senses the extra T4/3 , it turns off TSH production , so you see low TSH /high t4/3 results.
So base on TSH/fT3 evidence your daughter probably has the 'stimulating' type.. or at least enough of them to dominate over the other types.
If the 'blocking' type of TshRab were causing the positive TshRab result you would see a different pattern... because they 'block' TSH from working on the thyroid . so it produce less T4/3, and the pituitary notices the low T4/3 and TSH rises, and keeps rising because the thyroid is still not producing enough T4/3 since the TSH is still blocked from working on it.
So 'blocking' TshRab actually give results of high TSH and low T4/3, ie. a form of hypothyroidism .
The complication is you can't easily test them separately from each other, So you have to go by the effect they are having. Also it's not always the case that you have either stimulating or blocking antibodies (or the other 'neutral' type that don't do much)... presumably like everything else thyroid .. it's messy and you might have both, and the numbers of either might go up or down , showing different effects depending on which dominated at that time.
However as far as i understand , just 'having graves' does not mean it always need treating, it can be mild and if it is you have to weight up the benefits of treating it or not. PurpleNails say's there might be a benefit to calming it down early,, and she knows a lot more than me about it.. so i'm not saying don't treat it if it's mild .. just that you don't absolutely have to.
As for antithyroid medication .. no it doesn't exactly treat the autoimmune cause of graves .. it simply blocks the production of more T4 and T3 by the thyroid. The higher the dose the more it blocks but once you stop taking it, the thyroid can make as much as it normally did before.. assuming the antibodies go down enough to leave it alone.
Thanks for the explanation. Really clear
When my levels were found to be overactive they waited 8 weeks, had another blood test, then these were more overactive so I was then put on the Carbimazole.
I thought this was normally the process rather than putting on meds straight away but I think even on my first blood test the T4 was over range. The no symptoms part doesn't mean too much as there is some delay to see effects so if it is left overactive and it keeps going that way then indeed symptoms can come along and have risks to the body like thyroid storm as the extreme case.
Even though I say I had no symptoms there were some noticeable things like going for number 2's more than what was normal for me, so she may well be having some symptoms without realising. Plus I've always been slim but I felt like I did feel even slimmer than normal.
I must say Carbimazole brought my levels into normal range quite quickly in a few months. I've been on them since Dec 2020 and latest results now TSH 1.25 (From <0.05), T4 16.2 (was around 30 at the highest) and T3 now 5.8 (From around 10 at the highest) so the nurse is happy with this and says if still ok Dec I can come off. You have blood tests every 6-8 weeks so they can tweek the dosage to make sure the range is going the right way, I am just on 5mg now but started on 20mg. Most people are on this medication 12-18 months. With it being auto immune it can flare up again anytime but they would still test the thyroid I think yearly to keep track of it.
Thanks for the info.No changes in bowel habits, weight or appetite either.
Do you have Graves? Do you do anything to control/treat the Graves itself (dietary measures, supplements, etc)?
Am I right in thinking that while lowering thyroid hormones, Carbimazole doesn't have an effect on the underlying autoimmune cause, i.e. Graves ?
That is right auto immune means it is the bodies response, so medication helps to treat to make the levels right again. They said I have underlying graves and I don't do anything new in terms of diet/ supplements or anything but they say I've responded well to the treatment.
I eat healthily, I probably should look into getting a vitamins test but I'd have to pay for this myself, when I joined here people said get this tested, this and this it can feel rather mind boggling but I've always been someone who believes in a balanced diet so I would not go gluten free. I do take omega 3s but this is more for my bones as I have scoliosis as it's meant to be good for your bones/joints. I'm a bit skeptical of some supplements I'd rather look at getting what I need from food, unless I do a test and find I do need more of something specific.
My daughter has scoliosis too by the way. Single lumbar curve. Doesn't show. Not much pain. She does Schroth and physio for that.Great to hear that your thyroid levels are normalised. Is this the antibodies levels too? I assume that they are going to take you off the med and hopefully you won't have a relapse in the future (so they will be monitoring you for that).
Did you do the test (scan) where they use contrast to ascertain that the cause of the thyroid issue was Graves?
ah thanks I will have to look up Schroth, I have around at least 30 degree curve it does show a bit, I am a bit wonky lol but I just had the xray years ago, one physio session and that was it. I didn't have any pain so no need for continued physio. I need to take more care of my back as I am getting achy hands and always suffer with tense shoulders, a doctor mentioned carpel tunnel once which I suffered from in uni when my hand froze :/ I think it is flaring up a little again
I've had aches over time but I always see this as aches as there is a difference between pain and aches. Does she pay for physio privately? I'm kind of wary going to the GP just for a few aches I put up with when services are under so much pressure atm
I didn't have any scan on my thyroid at all and antibodies just tested once
My daughter's curve is bigger that yours, but lumbar, quite flexible, with little rotation hence doesn't show to the naked eye (very clear on x-rays though) and doesn't cause much pain. Schroth is good to keep flexibility and avoid a worsening of the curve (sometimes it can also slightly improve it). Unfortunately it's not available on the NHS so I have to pay for it.She has recently started physio sessions at RNOH, after several months on the waiting list. This is on the NHS. Both useful.
Yes, having to pay for vitamin tests is an additional cost. Not easy to do, but health is important. Again, it should be available on the NHS. It'd probably be cost effective too in the long term, because it could mean prescribing fewer drugs, which are expensive.
I was asking about the contrast test because somebody else pointed out that that scan is the only one which can fully ascertain whether the cause is Graves.
If you have taken the medication for a while, I think it would be fair to have antibodies tested again to see if the Graves is improving. Taking care of your health is important.
Thank you ") I've never actually had the curve measured it may be higher, and in my upper back with some slight rotation, so I am lopsided/wonky waist but you can only tell if I wear a bikini, I don't wear tight fitting clothes. I will definitely look into some more help with it . When I had the xray they said in 10-15 years time I could start to get arthritis in the spine but it has now been 16 years (I am 35 now) I really need to start doing more to avoid issues further down the line! My antibodies were "weakly positive" they were only ever so slightly out of range, I didn't think they would change much? I will ask at my next appointment
I've never actually had the curve measured it may be higher, and in my upper back with some slight rotation, so I am lopsided/wonky waist but you can only tell if I wear a bikini, I don't wear tight fitting clothes. I will definitely look into some more help with it . When I had the xray they said in 10-15 years time I could start to get arthritis in the spine but it has now been 16 years (I am 35 now) I really need to start doing more to avoid issues further down the line! My antibodies were "weakly positive" they were only ever so slightly out of range, I didn't think they would change much? I will ask at my next appointment
Not what you're looking for?
You may also like...
VERY confused...can positive covid test affect thyroid levels?
was fully recovered from covid. In hindsight I now suspect that prolonged covid symptoms was in...
Does The Thyroid Affect Potassium Levels?
low (3.2 range 3.5-5.3)
My TSH is 3.06 (range 0.27-4.20), which I think is a little too high...
Can an Hysterectomy affect the thyroid?
suggested that her Thyroid stopped functioning within 12 months after removal of her ovaries 20...
How much smoking affects thyroid levels?
the impact? Lower tsh with normal t4/t3 or?
My friend spontaneously told me about her other friend...
Can the tsh level affect u mentally? When ft4 is high?
mentally since tsh went above 1 can the tsh level affect u even though ft4 is still high?. iv...