Hiya, my first time using thriva, any help and advice with these results please
Help... understanding vitamin results please - Thyroid UK
Help... understanding vitamin results please
Written by

Kh1979
To view profiles and participate in discussions please or .
7 Replies
•
Hi Kh1979 I have looked at your 'page' and you only give your name. Is it possible you could add a little bit of history of your journey to finally being diagnosed. ")
Other members will be along soon to give helpful advice.
Hiya, I was diagnosed with hypothyroidism last year, tried different dosage of levothyroxine. Recently gp lowered my dose from 100 to 75, I generally feel well. I still have very slight numbness in my toes and hair loss but overall feeling ok.
Last results on 100mg was tsh 0.05 & t4 19.9, waiting for more tests since lowering levothyroxine to 75 which won’t be for another 3 weeks.
Taking Vit D supplements & multivitamins but unsure if I need to increase or start other supplements.
Thanks xx
SeasideSusieRemembering
Kh1979
I don't know if you're aware, but with your Thriva account there is a link to a pdf version of your results which lists them and if you post that it will show everything like this:
healthunlocked.com/thyroidu...
Did you have thyroid results with this test? If so what are they?
Last results on 100mg was tsh 0.05 & t4 19.9
What are the reference ranges, particularly FT4?
Why was dose of Levo reduced?
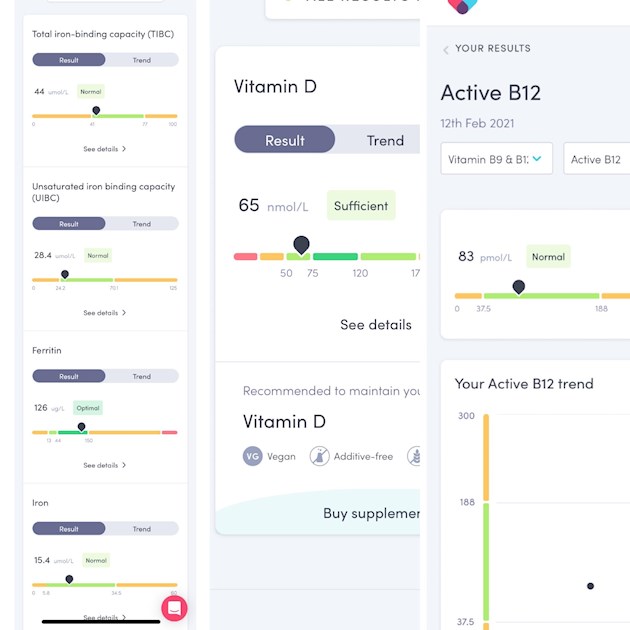
Vit D: 65nmol/L
This is too low. What dose of D3 are you taking?
The Vit D Society and Grassroots Health recommend a level of 100-150nmol/L.
To reach the recommended level from your current level, you could supplement with 3,000-4,000iu D3 daily, along with D3's important cofactors - magnesium and Vit K2-MK7 - do you take these?
Active B12: 83
Not too bad, Active B12 below 70 suggests testing for B12 deficiency so I would want my level to be over 100.
Ferritin: 126 (13-150)
This is a nice result. Ferritin is recommended to be half way through range, although I have seen it said that for females 100-130 is a good level. I'd be very pleased with this result.
Serum iron: 15.4
I think the range is 5.8-34.5. Serum iron is recommended to be 55-70% through range with the higher end for males. Yours is 33.45%. I wouldn't lose any sleep over this but just in case your ferritin is elevated due to infection or inflammation I think I'd repeat the iron panel in 3 months.
Was transferrin saturation included with this test?
Kh1979
Edited to add the following:
Were B12 and Folate tested?
Multivitamins aren't recommended here. They tend to contain too little of anything to help low levels, usually contain the cheapest, least absorbable and wrong form of ingredients, and often contain things we should test for first before supplement, eg calcium, iodine. If they also contain iron then this affects absorption of everything else.
Thank you so much for your help
Ranges
Tsh 0.05 (0.5-5)
T4 19.9 (9/22)
Gp lowered my dose to 75 as he said the tsh was to low, symptom wise nothing has changed since lowering my dose I feel the same as I did on 100 generally ok.
Mainly my symptom is hair loss so I’m thinking is that now down to vitamins etc?
Currently taking 1000iu Vit D, so will definitely increase this as you suggested.
No I don’t take magnesium and Vit K2-MK7, what do you recommend ?
My total B12 was quite high, is active b12 a different supplement? (Sorry I’m very new to all of this lol)
So you don’t think I need to add iron supplements?
Transferrin was 35% ?
Sorry for all the questions x
Kh1979
Tsh 0.05 (0.5-5)
T4 19.9 (9/22)
Gp lowered my dose to 75 as he said the tsh was to low, symptom wise nothing has changed since lowering my dose I feel the same as I did on 100 generally ok.
Your GP is making the same mistake as most doctors, in that he is adjusting dose by the TSH result and not the actual thyroid hormone result. FT4 and FT3 are the thyroid hormones. TSH is a signal from the pituitary to tell the thyroid to make hormone if it detects there's not enough. When we take exogenous thyroid hormone the pituitary senses this and unless we are taking too little then the pituitary is happy and doesn't have to send the TSH signal so it stays low.
If you don't have any symptoms returning, and are happy to stay on 75mcg then that's fine. However, if further down the line you find symptoms coming back (it tends to take at least 6-8 weeks for levels to stabilise after a dose change) then you may find that the lower dose isn't right for you and you are better with the 100mcg.
It's important to retest after any dose change, so make sure that you are tested 8 weeks after your dose was lowered to see how your levels have changed and how you feel.
Another thing to look out for is change of brand. If you have been given a 75mcg tablet is this the same brand as you normally have? Brand changes aren't a good idea, if you are happy on your usual brand it's best to stick to it. Again, retesting after a brand change should be done after 8 weeks.
Dr Toft, past president of the British Thyroid Association and leading endocrinologist, states in Pulse Magazine (the professional magazine for doctors):
"The appropriate dose of levothyroxine is that which restores euthyroidism and serum TSH to the lower part of the reference range - 0.2-0.5mU/l. In this case, free thyroxine is likely to be in the upper part of its reference range or even slightly elevated – 18-22pmol/l. Most patients will feel well in that circumstance. But some need a higher dose of levothyroxine to suppress serum TSH and then the serum-free T4 concentration will be elevated at around 24-28pmol/l. This 'exogenous subclinical hyperthyroidism' is not dangerous as long as serum T3 is unequivocally normal – that is, serum total around T3 1.7nmol/l (reference range 1.0-2.2nmol/l).*"
*He recently confirmed, during a public meeting, that this applies to Free T3 as well as Total T3.
You can obtain a copy of the article by emailing Dionne at
tukadmin@thyroiduk.org
print it and highlight question 6 to show your doctor if he is unwilling to look at FT4 and FT3.
Mainly my symptom is hair loss so I’m thinking is that now down to vitamins etc?
Low ferritin can be a cause of hair loss, your current ferritin level isn't a problem. However, other vitamin deficiencies that can cause hair loss are discussed here:
hubpages.com/health/16-Vita...
No I don’t take magnesium and Vit K2-MK7, what do you recommend ?
D3 aids absorption of calcium from food and Vit K2-MK7 directs the calcium to bones and teeth where it is needed and away from arteries and soft tissues where it can be deposited and cause problems such as hardening of the arteries, kidney stones, etc.
D3 and K2 are fat soluble so should be taken with the fattiest meal of the day, D3 four hours away from thyroid meds if taking D3 as tablets/capsules/softgels, no necessity if using an oral spray.
I like Vitabay or Vegavero K2-MK7
Magnesium helps D3 to work. We need Magnesium so that the body utilises D3, it's required to convert Vit D into it's active form. So it's important we ensure we take magnesium when supplementing with D3.
It's not possible to suggest a magnesium supplement as it comes in different forms, check to see which would suit you best and as it's calming it's best taken in the evening, four hours away from thyroid meds if taking magnesium as tablets/capsules, no necessity if using topical forms of magnesium.
naturalnews.com/046401_magn...
drjockers.com/best-magnesiu...
If you find that magnesium citrate is the form best suited to you then I like Natural Calm Original magnesium citrate powder, you start low and build up to a dose that alleviates the constipation without causing diarrhoea.
My total B12 was quite high, is active b12 a different supplement? (Sorry I’m very new to all of this lol)
They are different tests. The Total B12 measures the amount of B12 that is bound and unbound (free/active). A good Total B12 doesn't necessarily mean a good Active B12. The Active B12 test measures what is free/active and available to be taken up by the cells, it is considered to be the better test.
So you don’t think I need to add iron supplements?
Transferrin was 35% ?
Transferrin saturation is recommended to be 35-45% with the higher end for males, so yours is fine.
Serum iron, transferrin saturation and ferritin are the tests that are considered to be the important ones in an iron panel. Although your serum iron is a little lower than optimal, your transferrin saturation and ferritin are good. Iron supplements aren't recommended to be taken unless prescribed and regular monitoring takes place. I'm not medically qualified but I don't think you need to take iron tablets, but as I said I would repeat the iron panel in 3 months to see if anything has changed. If they go too low I would discuss with your GP.
Sorry for all the questions x
Don't worry, it's where we all start
Folate was optimal 45nmol/L which said very good on my report
Total b12 535
pmol/L. It’s just the Active B12 which was lower
Folate is fine. I've mentioned the Total B12 test in my previous reply.
Not what you're looking for?
You may also like...
Help understanding Results please
Hi Everyone,
Would really appreciate some advice, diagnosed with B12 deficiency last year and...
Help understanding blood results please
Hello,
Blood results are being questioned by my go. I have been taking Thyroid S for nearly two...
Help with understanding results please
Hi All – I am new to this board and hoping you may be able to help me, I am going through some...
Help understanding results
On 22 Feb I had blood test with NHS and it came back
free t4 - 10.5
TSH 5.30
Thyroid peroxidase...
Need help please understanding blood results
Hi everyone. Not posted before so hope it’s ok to ask. I really want to feel better & hope someone...