The advice and guidance we get seems utterly random at times.
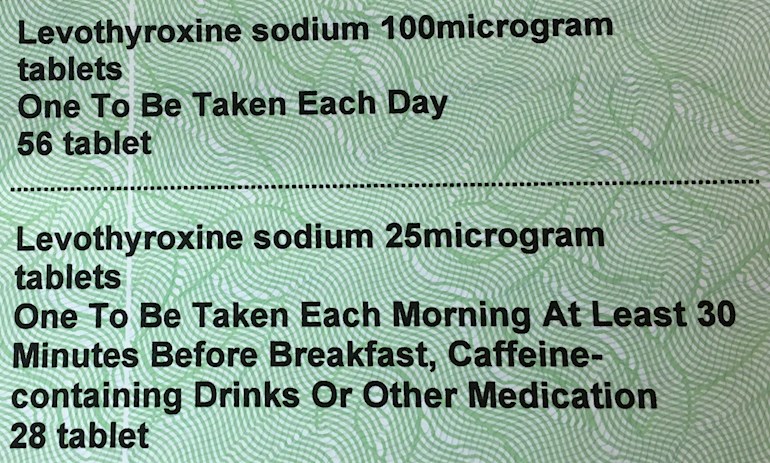
Take my most recent prescription. The 25 microgram tablet has to be taken in the morning, 30 minutes before breakfast, caffeine-containing drinks or other medicines. But no such instructions about the 100 microgram tablet! I can only assume that the instructions are, in fact, arbitrary.
(Also, the 25 microgram tablets are prescribed to make my dose up to 112.5. But the instructions say to take one a day. Someone needs to brush up on their logic and arithmetic.)
Written by
helvella
Administrator
To view profiles and participate in discussions please or .
On mine they are often totally different form of words, capitalization and everything. I guess someone just types into a database at some point, and then it keeps getting automatically printed onto different people's prescriptions, never getting checked or even read by anyone.
I think yours must be a particularly good quality example, considering how many people go decades not being told to have it away from food!
Ha! Its no wonder patients get confused by such instructions
Recently a GP prescribed me my ndt meds stating take 3-4per day and gave me 100 tablets to last me two months!!! Clearly maths is not that GPs strong point!! Lol.....took me to point out the error to get it corrected.
They really get confused with NDT. I had one office write my Rx for what was supposed to be 2.5 grain tabs for 90 days, or 90 pills. They sent it to the pharmacy as 180 tablets. It's a good thing we don't listen to them blindly...
Pinkpeony I started off with levo but it didnt work, next came levo and t3 which was better but I got spikes on t3 despite splitting it so I then move to ndt. My GP would not prescribe it on the nhs despite it being recommended by a specialist. So I had to buy it myself. Two years on the GP agreed it did me good but would not prescibe. So basically I shopped around at other GP surgeries to find one that would & changed to them. I argued that on levo it was more expensive because of all the additional medications I needed to deal with the symptoms levo did not resolve. They agreed and have prescribed it since. Its all on my records. The one condition is that I am under the care of a specialist to manage the treatment.
When I was a student I worked as a cleaner in a large teaching hospital and remember seeing a paper pinned to a docs notice board about prescription wording on antibiotics and how patients interpreted them. It might say take 3x a day meaning equally divided over 24hrs, but many patients took it literally to mean during daylight hours or over 12 hours. The majority of patients were not taking the tablets correctly due to unclear instructions given on prescriptions. Recommendations were given with examples of clear and unambiguous instructions in plain simple language that would ensure patients knew how to take the tablet properly.
That was 1978...seems some things never change....
Before I got ill I was working on a research project about how doctors talked to patients during clinical trials.
The doctors are absolutely terrible at communication. I think mostly because they don't consider that to be part of their job. They're not interested in imagining the patients point of view.
20 years I've been taking levo. Never had instructions on how/when to take. It was only in Nov when after feeling sooooo poorly for aleast a year that I went to Gp with heart / out of breath etc. Gp was useless (did discover that I need Statins) when picking them up from chemist, had a long chat with the 'boy' dispensing and he suggested changing how I take levo. Now take when I wake. Usually 2 hours before anything. Stopped coffee, cut right down on wine! Heart and breath is great now. Still have episodes of unexplained dizziness / weakness/ lifelessness. Gp says it's in my head!!!
Why were you prescribed statins? Was your total cholesterol high? If so, this is most commonly associated with hypothyroidism in female patients and will readjust with correct thyroid hormone replacement.
I don't know if you've come across Dr Malcolm Kendrick, but he discusses CVD and problems associated with statins on his blog. You might find it interesting.
Bloods again mid Feb...will insist on having a print out. Have never actually been told the figures! Since finding this sight I feel more informed. Thanks all.
High cholesterol can be harmful to your health if left untreated. Fatty deposits can form on the walls of arteries and veins causing artherosclerosis and restricted blood flow to heart lungs and brain. Can also cause blood clots
The cholesterol hypothesis has been debunked. As a start, you could have a look at the blogs of Dr Malcolm Kendrick and Dr Zoe Harcombe for further information. Current medical practice is years behind, unfortunately.
Yes they make interesting reads but there are lots of hypotheses on whether statins are good or not or whether high cholesterol is directly linked or not. The argument still continues and while it continues high cholesterol is still a cause for concern particularly in individuals with other cor morbidities. I feel it’s always wise to keep an open mind. One size does not fit all. In the meantime the link below is an analysis of one study done in the US
Normally, I would agree with you, but saying that 'one size does not fit all' does not really apply here, i.e. whether or not a specific biological marker is a symptom, or a cause. In scientific method, once a hypothesis has been disproved, that's it for the hypothesis, even if conventional practice continues as before.
‘One size does not fit all ‘ in this case is reference to the fact that we are all individuals and as such we behave in different ways to the same health issue.
While there is still ongoing research and arguments to prove or disprove current practice Drs will continue to treat rather then not. My personal viewpoint is that if I had high cholesterol I would choose to try statins. If the side effects outweighed the benefits then I would stop however if my cholesterol levels reduced and there were minimal side effects then I would continue. Some of the research suggests that statins don’t necessarily work directly on high cholesterol but indirectly. It’s up to the individual to keep updated and then make informed choices with their healthcare provider. Coming from a family history of stroke and heart disease .. high cholesterol being one of the links between those family members I would choose to try treating along with other lifestyle changes. It’s a personal choice
Of course it's your choice. I have a very similar family history, but having examined the research which has disproven the notions that are still part of conventional thought and practice, I've made a different decision. I can't argue with scientific method, so I choose not to shoot the messenger when my previously held ideas are challenged, though it can be a disturbing process to rethink fundamental ideas about how to live, what to eat, and whether or not to take certain medications.
It is a very hard process and we can only make decisions that we think are the best for us personally. I do always research before making any decisions relating to my health. As individuals we won’t always agree. It’s always good to have a healthy debate though and I’ve enjoyed talking with you today
I don't think anyone "needs"statins. Did have you increased your B12 and started CoQ10 to compensate for them? Statins can cause the symptoms you are experiencing, esp muscle weakness.
I have the same instructions on my latest pack of 25 mg Levo tablets, but the 50 mg pack states take as instructed. I was planning to query this with GP at appointment next week. I always thought it was the GP who instructs the chemist what instructions to put on the packet. Most of mine say "Take as instructed". A few weeks ago the pharmacist asked did I know to avoid grapefruit and grapefruit juice while taking statins, first time this was mentioned after taking them for years. Luckily I hate grapefruit.
Statins should be taken late evening apparantly. I thought that levo should be taken well away from anything with calcium such as milk and hence yogurt. Do I interpret from the above wording that my cups of coffee are medicinal? First time I’ve heard that!
I settled on levo in the middle of the night, when I’m always up briefly.....
Levothyroxine should be taken away from any food. Particularly coffee, as that's one of the foods that's been specifically proven to disrupt it.
In the middle of the night is perfect, because when you read the journal articles they suspect that many hours away from food may be better than just an hour or two away.
I had my levo increased from 75 to 100 as TSH was above range(4.39). Increase was 12 weeks ago, retested 4 weeks ago and now TSH is 0.42, just in bottom of range. I also changed to middle of the night levo so now well away from anything that could affect take up efficiency. Dr was concerned that I might have anxiety and high heart rate if levo was too high. I’d felt better generally and he took my pulse. That was 52, so no white coat syndrome that day!! Dr then asked how much exercise I did (I walk about 30 mikes a week) and was happy to keep me on 100...
It would be nice to see the freeT4 and freeT3 as well as the TSH to get more of a picture. It's likely you'd feel even better on another increase, but unfortunately many doctors go by TSH alone. Often you'll need a TSH somewhat below range to feel well. Many members have it almost undetectable!
Anybody know why it is recommended that we avoid Grapefruit with certain meds. What exactly does it do? I know that you shouldn't take statins with thyroid meds because it competes for the thyroid binding globulin (TBGs), so the transport mechanism is reduced to each of the meds if your taking both. But what of grapefruit? What does that do?
What started out, for many of us, as a fairly simple "be careful of taking xxx with grapefruit" has become a massively more complicated subject. Sometimes the effect is minimal, sometimes in the opposite direction to that expected.
This link will take you to about 230 papers for which the full text is freely available:
Wow, well that was mind blowing, I had no idea. I am a great grapefruit (GF) eater and it seems that fortunately thyroid meds do not interact with GF. Some of the papers are very difficult for me to understand but I get the gist of the problem - GF inhibit absorption of many drugs which leads to an "unhealthy" concentration of that drug in the body. Such a concentration can reach lethal levels.
Thanks for the links and I apologize for redirecting the thread - it was probably late and I probably mumbled off a thought that was just passing through the top of my head after Scadman mentioned GF.
I'd say the papers would be very difficult for almost anyone to understand. The ones I tried (because I did try to find a simple review paper that would cover the ground yet be readable) were all difficult to read.
Grapefruit (and sometimes other citrus fruit - but not always the obvious ones) have complicated impacts.
as a nurse who does some prescriptions there are various options available when a practitioner prescribes a certain medication, they choose an appropriate one and because most of these medications are on repeat the wording does not get changed. when I was first prescribed it said for review in 3 months patient aware does may need to be adjusted or stopped, now I am fully diagnosed this is not the case but the wording has not been changed
My medications have started to come from a central pharmacy, rather than being dispensed by the local one (Boots). They arrive in a sealed plastic bag, with a label similar to that one. When they were dispensed locally, there were no such instructions.
I first got prescribed levothyroxine last year. I was started on the 25mg and all I was told was " take these same time every day, I'll see you in 6 weeks". Unfortunately the PIL in the box did not state anything other than take it daily so I was taking it with my breakfast and cuppa tea as most tablets are with meals. Until I over heard someone else saying half an hour either side of food. Then I got retested was moved onto 50mg and the leaflet stated half hour between tablet and food. I read on here alot that an hour was the best so I do that now. I did go to take vitimins too for a few weeks until a lady from work told me not to take them together on the morning either. It would be nice for the leaflet to have a little more info 😆
Can I just ask what people do on split doses about the fasting? My morning dose (take half of my meds) is definately a proper fast but I struggle with aproper fast the midday dose.... I dont notice any ill effects but am curious what other do.
I take mine in 3 doses I do what I described above, fast 2 hours before and 1 hour after. It means I often get a one hour gap to have my lunch in. I have that as my main meal, and a snack late at night after my final dose.
It means I don't get a chance to have snacks or any drinks besides water across the day. I don't miss those as much as I thought!
The hardest thing is social activity. Sometimes I'm invited for a drink or a meal and I have to change meds around to accommodate, which is sometimes impossible. Grabbing a cup of tea for a chat is almost always impossible without missing a meal, so I just have hot water at those times.
Guess thats why lots of us take them first thing as we wake.......though there is now evidence that its better to take them at night! However being on a ndt that doesnt work for me as the t3 content kept me awake! For a while took a small evening dose now back to first thing and midday to avoid the afternoon slump.
I had antibiotics recently and sensibly it said 'take one tablet four times equally spaced apart every 24hrs.' Maybe some people are listening? 🤗🤗
I think we should be glad that this advice is AT LAST being given out with our meds. I took thyroxine for 16 years without this advice so was under-medicated for all that time despite taking 275 micrograms per day.
My health deteriorated dreadfully over that time but I could have been so much healthier if I had been advised how to take my meds.
I could go on, strong steroidal medication prescribed by an ENT for a suspected nasal polyp for over two years, which completely disrupted my sleep/circadian cycle. I was referred to the ENT by the sleep clinic!
Just over 2 years ago I took hubby to A & E when he slipped in the stairs and broke his shoulder. The A & E doctor decided he was dehydrated and put him on the kidney ward for a week, on a drip. Took him off his anti-coagulants, blood pressure meds and diuretics that hubby took for Atrial Fibrillation. After 6 days on the ward he came out on Christmas Eve night with none of the meds we'd taken into hospital. His AF was out of control, his legs were so swollen with fluids that he couldn't get his trousers on, blood pressure sky high. Saw the GP two days later to get meds who was so shocked he said hubby was a 'dead man walking'.
All he'd actually needed was some potassium supplements to fine tune his electrolytes, due to the diuretic meds he was taking. Nobody bothered to look at his medical history.
Oh, and his broken limb? He did not see anybody from orthopaedics in all the time he was on the ward. His only treatment for a 'shattered neck of humerus' was paracetamol and a visit from a physiotherapist who badly fitted the wrong kind of sling.
Worse still, I had to take him back to the same A&E to get him seen by an Ortho. He needed an op on his shoulder but was too medically unstable to have the op. Needless to say, over two years later we are still waiting for treatment to be completed on his shoulder.
Doctors need to treat us holistically instead of just treating one symptom in isolation.
Re the break. One night my son turned up on the doorway asking if ok to stay the night-he stayed 4 months! He had a similar break and was operated on and ended up with 7 hefty screws in his arm and an awful lot of physio! So shocked at the 'treatment' you mentioned.
I'm puzzled as to why my GP who stopped my T3 and upped my T4 prescribed two 50 mcg tablets and not a 100mcg. What on earth would make the difference there. Unless there is a cost factor involved.
That might explain something that happened to me recently. after been constantly moved between 50 and 75 mg doses, a new GP prescribed a 50 mg tablet and a 12.5 mg tablet. When I took the prescription to Boots there is no problem getting the prescription fulfilled, but if I take to local small pharmacy they say the 12.5 dose is not available, when I said Boots had no problem getting them they said they use a different supplier. They suggested I take a 25 mg tablet on alternate days (didn't work out as I kept forgetting if I had took it or not) or I cut a 25mg tablet in half, had to purchase a pill cutter from Amazon as they are very small tablets anyway. After seeing my usual GP she has put dosage back to 75mg so problem solved for now.
Perhaps it's just that the 25 mcg tablets are sensitive little flowers who need their own space without other substances, whereas the 100 mcg ones are tough and don't care! (totally joking, of course.)
My belief is that as with so much else relating to our health issues we have to remember that we are all individuals with our own specific diagnoses and treatments. My daughter's current specialist was really surpised when she suggested that she had to wait at least 15 minutes before eating/drinking after taking her T3. She now has her T3 when she gets up followed by her first cup of coffee of the day. She is better now than she's been for years, but that could also be because she's now got a proper diagnosis from someone who actually knows what he's talking about as regards her medication as well as her diagnosis. I'd say disregard "what it says on the tin" and take your doctor's advice (as long as he's reliable). Jane x
I have always pointed out that there has been precious little proper research on what affects absorption of T3. Much of what is said is based on the assumption that T3 behaves similarly to levothyroxine. I suppose that is not an unreasonable place to start - but it is clearly ridiculous that is where we are.
I'd certainly not take my GP's advice! Can't actually imagine him discussing or making any comment on taking levothyroxine.
What a revealing post this is! If I was a doctor I would feel really embarassed that so little accurate guidance is given critical to effective uptake of thyroid medications. Difficult to comprehend why.....
Thank goodness for health unlock & all the knowledgable wise ones on here or we would all be in the soup!! 😊😊
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.


") I have a very similar family history, but having examined the research which has disproven the notions that are still part of conventional thought and practice, I've made a different decision. I can't argue with scientific method, so I choose not to shoot the messenger when my previously held ideas are challenged, though it can be a disturbing process to rethink fundamental ideas about how to live, what to eat, and whether or not to take certain medications.
I have a very similar family history, but having examined the research which has disproven the notions that are still part of conventional thought and practice, I've made a different decision. I can't argue with scientific method, so I choose not to shoot the messenger when my previously held ideas are challenged, though it can be a disturbing process to rethink fundamental ideas about how to live, what to eat, and whether or not to take certain medications.  (totally joking, of course.)
(totally joking, of course.)