I was diagnosed with an underactive thyroid / hashimotos last year. I was prescribed Levo but had terrible side effects. I switched to thyrogold & lost a considerable amount of weight. In the last few weeks, my weight has started creeping up again. I am so so down about it.
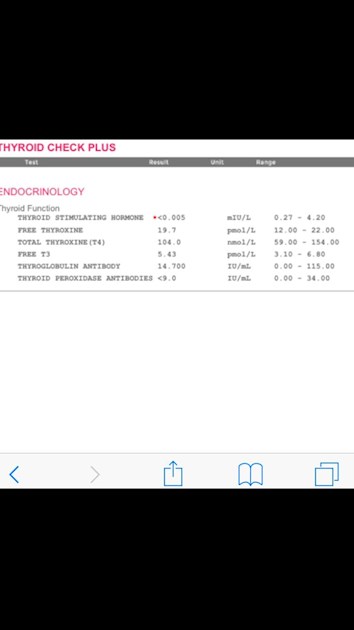
I decided to have my bloods done privately to get an overall picture of my thyroid health.
Can anyone advise whether I can add T3 or increase my thyrogold due to the weight gain. I currently take 4 150mg capsules every morning. Thank you in advance
Written by
Hippyhappy234
To view profiles and participate in discussions please or .
I'm not that familiar with thyrogold but assume it is the bovine NDT which is weaker than porcine. Is it Dr. Lowe's formula? Your levels actually look good but you could still increase something. I think T3 is an excellent hormone for some of us to take. I've done T3 only in the past and did very well with it. The only thing about the bovine source is that you need such a high dose compared to porcine, right?
I am no expert with NDT, but wonder if splitting your dose to take it two or three times a day would maybe help. Hopefully others with experience of this will comment.
looking just at the blood levels you posted and comparing them to research and 'authoritative' endocrinologist society views it seems you may be over replacing T4 Somehow or other! Treated T4 levels are more frequently settled at 13-15 and TSH way to low for straightforward hashimotos ... have you been advised to completely suppress TSH? Otherwise it’s generally regarded better around 1.0, your free T3 may be a little too high too. T4 Treated levels from large studies I have seen achieving TSH around 1.0 are ft4 at about 15 and ft3 about 4.....
If 'authoritative' endocrinologist society views were valid there would be no need for thyroid fora. Suppressed TSH does not mean overmedication when FT3 remains within range. Neither T4 nor T3 are over replaced because they remain within range.
Healthy euthyroid patients generally have TSH 1-2, FT4 mid-range and FT3 just below to mid-range. Patients optimally dosed on Levothyroxine will hav e lower TSH and higher FT4 and FT3.
Dr Toft, ex-President of the BTA, states in Pulse Magazine, "The appropriate dose of levothyroxine is that which restores euthyroidism and serum TSH to the lower part of the reference range - 0.2-0.5mU/l.
In this case, free thyroxine is likely to be in the upper part of its reference range or even slightly elevated – 18-22pmol/l. Most patients will feel well in that circumstance.
But some need a higher dose of levothyroxine to suppress serum TSH and then the serum-free T4 concentration will be elevated at around 24-28pmol/l.
This 'exogenous subclinical hyperthyroidism' is not dangerous as long as serum T3 is unequivocally normal – that is, serum total around T3 1.7nmol/l (reference range 1.0-2.2nmol/l)."
Results of patients taking T4+T3 combination treatments will usually deliver lower TSH and FT4 than patients taking Levothyroxine only because higher FT3 will suppress TSH and FT4.
Are you saying learned and experienced endocrinologists views are invalid? Everything in the range of the debate is valid for consideration unless it is factually absurd and or lacking in sufficient evidence or theoretical possibility to even warrant further investigation.
A substantial body of recent research points to individual set points of thyroid homeostasis being defined by at least free T3, free T4 and TSH. Lab normal ranges of individual hormone levels are not necessarily the yardstick for optimal hormone replacement. Steady state, sustainable, reasonably risk and symptom free managed thyroid homeostasis is the holy grail of replacement therapy and the statement 'The appropriate dose of levothyroxine is that which restores euthyroidism and serum TSH to the lower part of the reference range - 0.2-0.5mU/l.' is possibly over simplistic and over generalised.
Sticking to the paradigm that patients should expect that Levothyroxine replacement therapy will morph euthyroid blood levels into different part, of the Lab ranges and thereby define appropriate treatment ignores all the people who do this and still feel unwell or suffer side effects. It also ignores the possibility that empirical euthyroid blood levels are a valid target for replacement therapy . Achieving these levels with Levothyroxine alone may indeed be unrealistic - hence the debate on more subtle combination replacement therapies.....
It often seems prescribers are overly reliant on ramping up Levothyroxine doses to meet patient frustration about symptoms and end up with unecessariIy and perhaps unhealthily low TSH and unecessarily high free T4 to pump up free T3. Some individuals may have genetically lower or higher set points for T3 which were never known before they became athyreotic. It may be reasonable to suggest there is no such thing as 'unequivocally normal' T3.
It may be that some of the frustrations of treatment come from excessive free T4 and overly suppressed TSH. And then there are the considerations of valid opinions based on valid research that suppressed TSH can have long term health risks:
Dr Graham Leese, from Ninewells Hospital and Medical School, led a research team examining patients on thyroxine replacement therapy. They studied how variations in these patients’ TSH levels affected their long-term health. The study followed 16,426 patients taking thyroxine (86% female, mean age 60 years) and examined how their risk of contracting a range of diseases varied with their TSH levels.
The study found that patients with very high (>4.0mU/l) or suppressed (≤0.03mU/l) TSH levels more frequently suffered from heart disease, abnormal heartbeat patterns and bone fractures compared to patients whose TSH levels are in the normal range (0.4-4.0 mU/l). Patients who had a slightly low TSH level (0.04-0.4mU/l) did not have an increased risk of contracting any of these conditions.
Are you saying Dr. Toft, consultant endocrinologist and ex-president of the BTA views are simplistic?
I'm saying some endocrinologists are neither learned nor experienced re thyroid. Amongst them I include those who think TSH is the gold standard by which thyroid levels are judged and that FT4 and FT3 are unnecessary; those who dose solely by TSH levels; those who think FT3 levels below range are unimportant; those who do not accept that Levothyroxine can cause adverse symptoms; those who say Liothyronine is a placebo, those who tell patients on Levothyroxine that their symptoms are psychological and nothing to do with thyroid when the patient's TSH is >6 and they are clearly undermedicated; endocrinologists who claim a patient was never hypothyroid at diagnosis without seeing their thyroid levels at diagnosis and take them off replacement, discharge them, and then GP has to re-refer when TSH rises, etc. etc.
I have read research re suppressed TSH causing AF and osteoporosis with interest. The Rotterdam Study finds no association between TSH and atrial fibrillation and a meta-analysis of fractures in patients with TSH <0.1 found one extra hip fracture per 1,000 patient-years.
My TSH has been suppressed <0.01 post thyCa. Endo would like it less suppressed at 0.05. Three dose reductions didn't budge TSH but FT4 and FT3 dropped considerably so it seems likely my TSH set point has been reset. I declined further dose reductions in favour of feeling well today as opposed to increased risks of adverse health in the future.
I was saying that statement you referred to may be over simplistic and over generalized, and there’s evidence to suggest that; I don’t know enough of dr Toft to have formed such a sweeping opinion about all his views;). And I agree with all of your views expressed in your second paragraph, I’m no fan of any of the half dozen nhs and private specialist endocrinologists I have seen or of the reports and opinions promulgated from others. Having said that I don’t write them all off and as I said in my previous reply, regard all views as valid for consideration in the discussion unless they are obviously ill founded lacking in evidence or lacking basic theoretical consistency with thoroughly established understandings.
Hi, Are you 100% certain about the Hashi's diagnosis? I'm no expert on NDT, so can't help you with dosing, but your antibody levels are really low and your TSH is suppressed to what could be considered hyper levels. Have you had pituitary issues looked into? There are people on this forum who have them and may be able to tell if it's worth you looking into them..
If antibodies were high when Hippyhappy234 was diagnosed then it is autoimmune (Hashimoto's). If not, then it's not Hashimoto's which caused hypothyroidism.
TSH is very suppressed, FT4 is in the upper range and FT3 is just shy of the upper third of range, so you appear to be optimally dosed on 600mg. Thyroid antibodies are negative for autoimmune thyroiditis (Hashimoto's).
If you are still symptomatic you could try an additional 1/2 capsule of ThyroGold. It's important to keep FT3 within range.
Neither ThyroGold nor T3 are weightloss aids. If that is your main reason for wanting T3 you should be aware that overmedication can cause weight gain.
Have you made modifications to your diet? Gluten free? Lots of good fats fruit and veg? My understanding is not to restrict calories but eat lots of protein good fats and fruit and veg. Cut out processed foods and sugar?
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.