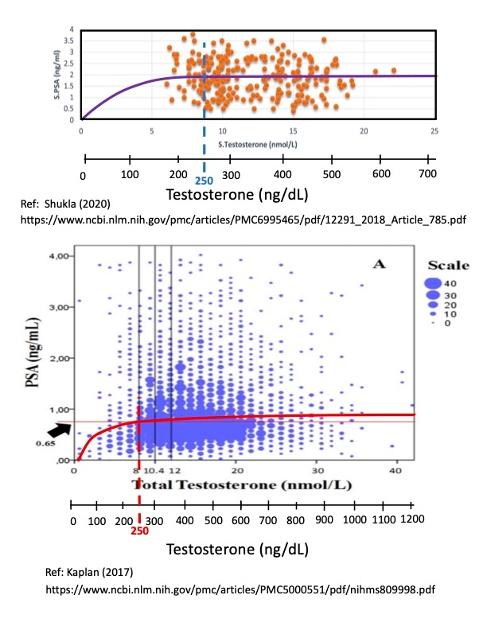
Here are two plots comparing PSA values to Testosterone levels taken from a pair of large data sets.
What is striking is the large amount of scatter in the individual data from both datasets, with factors of 2-6 X deviations from the average (or median) values. The upper plot has N = 255 data points (Shukla, 2020), and the lower plot has N = 2967 data points (Rastrelli, et. al, 2013, reproduced in Kaplan (2017)).
Both plots have been fit with an average linear-flat curve that is based on Morgentaler's Saturation Model. At the theoretical limit of zero testosterone, there is no "food" for feeding prostate cancer cells, and the corresponding PSA value is theoretically zero, which anchors the curve fit the origin at (0,0).
Note that the linear regime only appears to be present for T 250 ng/dL (as indicated by the vertical dashed lines). Morgentaler wrote that the rollover point was "from 240-250 ng/dL", which agrees very well with the observed saturation points of these two data sets.
The are three key takeaways:
(1) Below about T = 100 ng/dL there is a linear relationship between PSA and testosterone, meaning, for example, that a 50% drop in testosterone implies that there will be a similar 50% drop in PSA (all other factors being equal). This is relevant for castrate-sensitive men who are doing ADT, namely that lower T is better because this will cause a lower PSA;
(2) At T > 250 ng/dL, the PSA becomes "saturated" at a maximum average value of about 0.65 to 1.8 ng/mL, and any increase in Testosterone greater than T= 250 ng/dL will not increase the PSA level any further. This is an important result for castrate-resistant men who want to supplement their T level (for example, from 200 to 1000+ ng/dL) after completing their ADT treatment cycle. According to this data, supplementing T levels from 200 to 1000+ ng/dL will have no effect (no increase) on their PSA value.;and finally
(3) There is tremendous scatter in the PSA data (factors of 2X to 6 X).
Bob
Written by
janebob99
To view profiles and participate in discussions please or .
Bob, you seem to very analytical in your approach. I like. Have you given any attention to BAT studies? It dovetails with Testosterone and modulating between high and low.
Yes, I like analyzing data and plotting it to see trends. I hate long tables of numbers. It's too difficult to pick out what's important.
Glad to be of service!
In my plots of PSA vs T, I have included some data from BAT studies. Not all of them report PSA vs T, but some do. I think there's a lot to be learned from the BAT protocol and responses.
Thanks, Anomalous, for taking the time to share your data. I will add it to my database.
If you think you're "cured", then it's probably OK to supplement your T to normal or high- levels. Morgentaler has written at lot about this situation.
Your PSA wiggles around an average of about 0.3 +/- 0.1, with no evidence of significant growth over the past 12 months. So, this would indicate you are likely "cured".
(Remember your docs are the experts....I'm not an MD).
How long were you Lupron?
Typically, there is a 2-4 month lag for the PSA response to a step change in T-levels. See attached plot for someone starting to use an estrogen patch, but the kinetics should be the same as for Lupron. The testosterone drops to castrate levels in 2-4 weeks, but it takes 2-4 months for the PSA to drop to 10% of baseline PSA.
If you believe Morgentaler's saturation model, then PSA is independent of Testosterone for T > 250 ng/dL. I posted some new plots earlier today that support that model very well. You should be safe to keep your T high. In your when you had two spikes in T, there was no big spike in PSA because the T-levels were high (> 400 ng/dL). Perhaps a small bump 2-3 months after the T peaked.
If your PSA starts to rise again, and exceeds 2.0 then that would be considered a PSA Failure or PSAA Recurrence. Checking the doubling time in that case would be important. DT's less than 8-9 months would indicate a growing tumor.
Here's a cross plot of your PSA vs Testosterone. It fits nicely with the Morgentaler Saturation Model, with a deviation from linearity at T = 300 ng/dL, and a rollover/saturation point at T = 400 ng/dL. But, I didn't force the curve to go through the origin. The curve is shifted to the right by about 100 T-points. But, the basic shape is right on.
Here's your data (green triangles) added to my collection of points from about 10 different data sets. I normalized the PSA data to the % of the maximum/peak value (which is at 100%). Doing a normalization is valuable because some of my PSA values are as high as 2500 (indicating a large number of Mets). The solid red line is my best eyeball curve fit to the data, which fits Morgentaler's model almost perfectly with a rollover point of about T = 300 ng/dL). The large scatter indicates that there are many different stages of PCa included here, from Active Surveillance (low PSA values) to extremely high PSA's with lots of mets.
There's a lot of PSA scatter in your data, maybe because you used 3 different test labs. It would be interesting to plot data from just one lab at a time, to see if the scatter goes down...
So as I’ve posted before, I’m using three.1mg patches changed weekly plus one daily 80mg. Xtandi tablet. My T is very low (<3.0) and psa is undetectable (<.1). I wonder if I let my T increase would I have more strength and endurance and still keep my psa in check. Even if psa rose a bit would it be worth it to feel better? Are there any clinical trials that could tell me the answer?
I'm not aware of any trials that address your questions. Assuming that you are still castrate-sensitive, for best outcomes you want to have T as low as possible. See attached Survival plot.
The downside of estrogen therapy and castration is reduced muscle mass and strength, gynecomastia, and increased risk of breast cancer (especially if you are BRCA 1/2 positive).
As to your question about increasing T, you could add T, or cut back on your number of patches. It a great question to discuss with your MO.
It's the classic trade off between QoL and survival outcomes, as you well know. Would having stronger muscles be worth going from 90% survival probability down to 85% ? (I just using this as an example..). That's the tradeoff.
I worry that increasing your T to 20-50 ng/dL will reduce your survival probability by a large amount (according to this plot). And, would increasing T to 20-50 ng/dL be sufficient to improve muscle strength/mass? It's such a small absolute increment going from < 3 ng/dL to 20-50 (relative to a normal level of 500 ng/dL) that I doubt it would have much impact on muscles. There are papers where they gave men high doses of T (up to 3000 ng/dL), which did improve leg strength, endurance, etc. But, you are very far from those numbers.
If your life is miserable because you are a runner and can't run, or a prof. footballer, etc. then it might make sense to increase T and not worry about having a potentially shorter lifetime.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.