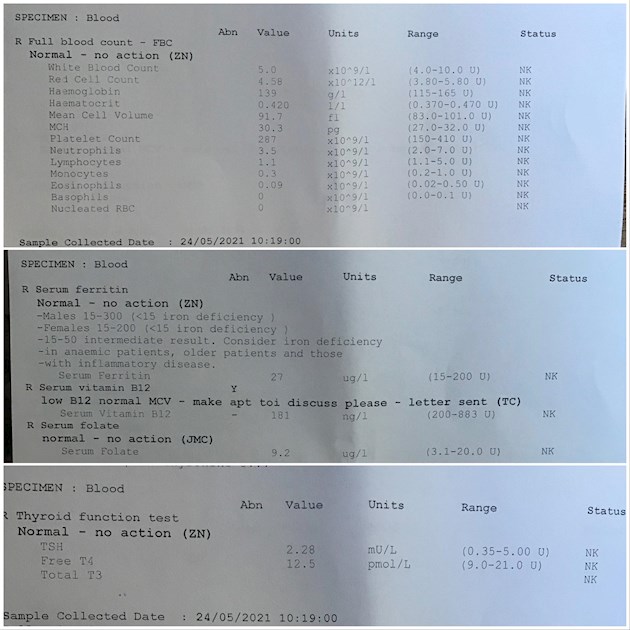
So due to my recent blood results, my doctor ordered a b12 antibody test (Intrinsic factor I think). I had a look at my recent bloods, and as far as I can tell my b12 is only slightly under range not by that much. Could these blood results suggest possible pernicious anemia? They seem normal enough to me. I have been getting muscle twitches for the last 2 years, mainly in my legs and face and have most recently been having horrible chest pains after I eat, bad indigestion I think. I also get a strange/funny feeling tongue, it kind of feels like I’ve burned it, and my gums have been bleeding excessively despite being on top of oral hygiene 🤷♀️ However I will preface this by saying I do have autoimmune hypothyroidism, so any symptoms I experience could be due to that possibly.
Thanks in advance for your knowledgeable input 😊
Written by
XxAnyaxX
To view profiles and participate in discussions please or .
Pernicious Anaemia is a bit of a misnomer.Pernicious Anaemia is actually an auto-immune disorder affecting the gut, and attacking the mechnanisms by which we absorb most of our B12.It was first identified a few centuries before B12 was identified as a type of anaemia which led to madness and death.
B12 is used by a lot of processes that go on in your cells - one is the process that produces new red blood cells - the consequences are a particular type of anaemia in which the red blood cells are larger and rounder than they should be. However, this isn't necessarily among the first symptoms to occur and isn't present in 20% of patients who are B12 deficient.
The symptoms of B12 deficiency develop very slowly - over years or even decades so they often creep up on you without you realising and it is only when you reflect back that you recognise them as symptoms.
They are far ranging because B12 plays a part in a lot of the processes that go in in cells.
If you have neurological symptoms then it is important that you get treatment sooner rather than later.
Serum B12 is a problematic test as a diagnositic tool for B12 deficiency as the normal range (which covers 95% of people) is enormous and people tend to sit at a particular point in the range, regulating levels using stores in the liver.
If you have an absorption problem, this will also affect the mechanism that the body uses to release the regulating stores and levels will start to fall.
This means that a significant fall (ie one that can't be explained by the margin of error = 20%, in the test) is an indicator of an absorption problem in a way that a single point test never could be an absolute indicator. This means that symptoms will always be important in evaluating a deficiency.
The stomach issues may well be a sign of low stomach acidity associated with PA but a potential B12 absorption problem in its own right.
Studies show a probability of 40-60% of someone with an auto-immune thyroid condition developing PA or a B12 absorption problem.
The following links may be of interest/use
a) re testing for PA/B12 absorption problems (and the results above make it unlikely you don't have an absorption problem)
You are probably aware that most patients being treated for hypothyroidism find that then need TSH to be around 1 whilst on treatment so may be that your thyroid problems are undertreated. Patients also report needing to reduce thyroid medication post starting B12 treatment.
Thanks for all the information, very interesting read. Ohh, after reading the first study, I remembered I have a genetic mutation of the fut2 gene. The gene variant I have means I have issues absorbing b12 if I remember correctly. I took a 23andme test a few years ago and it flagged up the mutation. Maybe this could explain my low vitamin b12 🤷♀️Who knows
according to this a variant on fut2 affects the bioflora of the gut which could lead to general absorption problems but the mechanism for B12 absorption is very specific so unlikely it would be the only thing affected in that casencbi.nlm.nih.gov/pmc/articl...
This article mentions a link with crohn's but only where you have two copies of the variant
The study about the possible link between FUT2 mutations and crohn’s is actually interesting. My Brother actually has crohn’s, and has many of the same FUT2 (non secretor) gene mutations as myself. We both did 23andme 😅 obviously I can’t infer causation completely, but it’s definitely interesting 🤔 Thanks again😊
When I had bleeding gums continuing after B12 injections were started, my GP tested my ferritin and folate, which were not below range but were low within range -low enough to possibly be likely culprits. My B12 level was not particularly low either: 196 ng/L (range: 197 - 771 ng/L) - but treated anyway because of symptoms .
She said that ferritin (range 13 - 150 ug/L) can cause symptoms below 60 ug/L. Mine was about 45. Later, an Oral Medicine consultant looking at my angular cheilitis (cracks at corner of mouth) and burning tongue, said he would prefer level to be 80 ug/L. A real struggle to get there and stay there, even with additional supplements. At lowest, it was 36. Now 82 and happy to be there !
Folate (range 4.6 - 18.7 ) also a little difficult to stabilise- was 5.5 at first. This level is optimal in top 1/3rd, I have been told.
Both of these can also give you problems if too high, so would need regular monitoring if supplementing.
I no longer get bleeding gums but it would be difficult for me to determine whether because of better folate or ferritin levels or better B12 levels- or all three required to get rid of this symptom since all were treated at about the same time. GP's suspicion was that low ferritin was the cause of this particular problem.
It will be even more difficult for you to disentangle symptoms - hopefully your GP can be of help with this and will be keeping a close eye on blood test results and direction of travel before deterioration causes further problems for you. Ask for printouts for reassurance that nothing is being missed.
Hi CherylClaire, yes you could be right in that my ferritin and folate are classified as in the “normal range” but are still low enough to cause issues. I may start to supplement my ferritin and folate then. Thanks 😊
Make sure that your GP regularly checks progress on that, XxAnyaxX - can be difficult to work out what is being effective and keeping levels stable, particularly with other conditions going on. Can take a while to get moving too. Far better that your GP gives you a course of supplements, at least initially - then more likely to include regular monitoring ! That way, they will be aware of any symptom relief or lack of it, too.
Treating low folate when B12 deficient can mean that it is more difficult to recognise the B12 deficiency as it will correct any anaemia without the lack of methylcobalamin being similarly addressed - so if your B12 does need repleting, this should be done before starting folate supplements.
Even now, my GP checks folate, ferritin, vitamin D and thyroid as well as FBC - just to be sure. This has been going on for six years and is usually yearly now -last one in Oct/Nov last year returned best results I've had so far. You know you're doing well on all other fronts when they start pointing out that your cholesterol is still high !
Find one GP who is willing to listen and investigate -then stick to that one. Continuity will prevent further entanglement and confusion about what best to do next.
Thanks for the reply 😊 I will see how I go with b12 supplements if I get any, otherwise I’ll buy some myself. Glad to hear everything looks good on your bloods 😊 Have you been diagnosed with pernicious anaemia then? Yes I think I’ll stick with the same doctor I have now she seems to be helpful, as she was the one who spotted my low b12 and ordered the antibody test. I assume if I hadn’t already been diagnosed with a autoimmune condition, she may have just put it down as dietary or something and not PA 🤷🏼♀️
Long as she's aware that 40-60% of those with PA test negative for PA. She at least knew about the test, so hopefully knows this, too. Medical advisory bodies are aware of this, the people who write guidelines for medical professionals, which is why there is such a thing as PA(abNeg). No PA diagnosis for me; I was just told at first that, since the treatment was the same either way, a diagnosis didn't really matter. Didn't even know there was a B12, so couldn't question anything, plus so ill. When I got worse after a few months of B12 injections, more tests were done. This is when functional B12 deficiency was diagnosed, confirmed by the hospital lab, and injection regime was altered to 2 a week.
My folate and ferritin were low, and vitamin D now on prescription because of osteoporosis of the spine and osteopenia of the neck. This was found by dexascan (bone density) automatically offered - not because of deficiency, because I'd broken both shoulders. Luckily not at the same time ! All of this, I'm sure, related. Your GP seems to have done all the right tests- but don't see vitamin D on there. I'd check if that has been done too.
Yes I had read that as well, I’m hoping she does. Oh right, well at least you’re getting treatment now. Gosh that sounds awful, hope you’re feeling a bit better now. If I remember correctly my vitamin D was 18.8 ( range 50-175) I’m not sure what it is now, that was just over a year ago 🤷♀️ My doctor wasn’t too concerned so I just supplemented with a mouth spray.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")