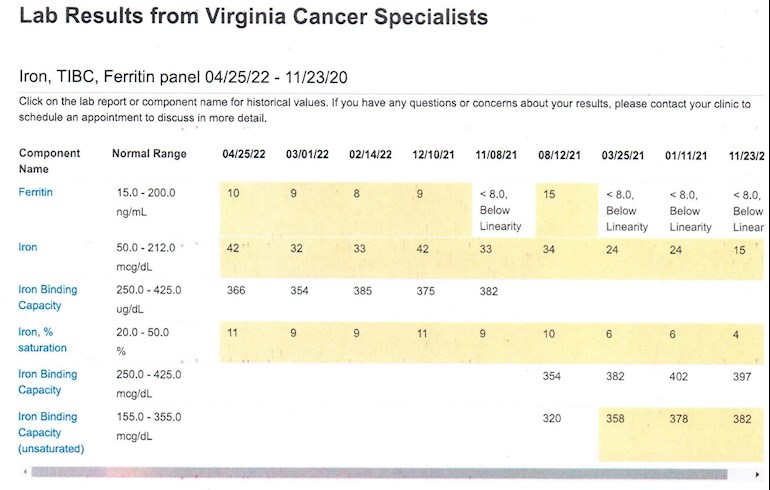
Thought it might be interesting to some to attach the actual numbers to what we have been discussing for those interested in what drives erythrocytosis and why iron levels matter. Deregulated iron metabolism is at the core of PV.
We have been discussing our treatment options on the forum, including Besremi dose titration and phlebotomy. I was using phlebotomy-only for a couple of years, until May 2021. The whole point of phlebotomy is to make you iron-deficient without anemia. Less iron = Less RBCs
Unfortunately, iron deficiency can have adverse effects. The iron deficiency symptoms got worse than the PV symptoms, That is why I started on Pegasys. Later switched to Besremi.
While the IFNs are doing a very good job controlling the erythrocytosis, the HCT has been creeping up. This is not because the IFNs are not working, It is because my body is restoring the iron levels over time. More iron = More RBCs. Over time, I anticipate needing more IFN to control the erythrocytosis. The strategy will be to carefully titrate the dose of Besremi to stay in a Complete Hematologic Response without unacceptable adverse effects.
As you can see from the chart, my iron levels are indeed steadily going up. This was also evident in the erythrocyte-related numbers on the CBC. I feel much better with the higher levels of iron in my body and the low iron AEs I was having have resolved. My HCT and PLT are far more stable on IFN than when I was relying on phlebotomy. Eventually I will reach a point of homeostasis, maintaining a reasonable iron level and controlling erythrocytosis and thrombocytosis with the right Besremi dose. It is all a balancing act.
We are learning together how things will really play out with Besremi and perhaps some other new treatment options. I hope others will also continue to share what they are experiencing so we can compare experiences. We really are stronger together.
Written by
hunter5582
To view profiles and participate in discussions please or .
Thanks hunter5582. In my case, platelets are in range, but HCT is yet higher, 48. I have been taking Besremi for 6 months. I yet take phlebotomies according to my HCT. It is usually each two months. I had some light side effects susch as dry mouth, a few moments of itching but with cardamom to mouth and organic essential oil it was out, also my strict diet, exercise, removing toxics of my life, no toxics relationships, etc. You know.
A question: my hemo dosen't check all the parameters you have in your iron graphic. Can you tell me the kind of test he orders for you. Referred to iron a blood profile is called here what my doctor ask for me each month.
It is called various things. Iron Panel, Iron-TIBC-Ferritin Panel, etc.
• Serum iron. This test measures the amount of iron in your blood.
• Serum ferritin. This test measures how much iron is stored in your body. When your iron level is low, your body will pull iron out of “storage” to use.
• Total iron-binding capacity (TIBC). This test tells how much transferrin (a protein) is free to carry iron through your blood. If your TIBC level is high, it means more transferrin is free because you have low iron.
• Unsaturated iron-binding capacity (UIBC). This test measures how much transferrin isn’t attached to iron.
• Transferrin saturation. This test measures the percentage of transferrin that is attached to iron.
The issue is that Ferritin only tells part of the story. It is a rough measure of iron that is in storage. Note that the normal range is from 15 - 200. You have to look at the other iron measures to fully see what is going on.
This is a presentation about iron physiology that you may find of interest.
Thanks Hunter, this is very interesting and backs up what/how I feel. Officially I'm only ET (PLTs 7/800 age 54 aspirin only) but my HCT can go up 48. Heam suggested trying venesections with HCT target of 45 to see if it helps with headaches and fatigue. Generally it does but it's a fine line when it comes to anemia. As per others ferritin isn't regularly tested. In April 21 I felt such a lack of energy I suggested I was anemic. So they tested and presented me with several boxes of ferrous sulphate and ferritin at <8 . Finding our personal sweet spot is the goal. I think mine might be to have a VS at 48. If I have a VS at 46 that's when anemia seems possible. This I found out to my cost after going on walking holiday in the mountains two days after a VS with HCT at 46. Long story short I couldn't walk up mountains. Two weeks later after self treatment with iron I'm a bag of energy. Even before any diagnosis I often found iron supplements helped when energy was low (I used to run 30 miles a week but no more - too many visual migraines)Final point and it's early days. Semi retirement may also reduce HCT. I hoping I'm proving the link with stress is real but I need a few more test cycles.
It is a bit hard to tell what is going on. It sounds like you are top of sorting this out. Iron deficiency can certainly cause fatigue even when you are not anemic. That was certainly the case for me. It was the consequence of using phlebotomy to treat the PV. I feel much better with my iron levels higher.
A few things to note. Iron deficiency can cause reactive thrombocytosis. If you have ET and iron deficiency, this can be an issue. The other side of this is that more iron can = more RBCs. If you take more iron your body has what it needs to make more RBCs. This why iron supplements are contraindicated for people with PV.
I believe there is evidence that stress can increase platelet production. I have not heard of it increasing erythropoiesis. Hypoxia definitely increases erythropoiesis. Spending time at elevation (less oxygen) will increase RBCs, especially if you are physically active. Please do let us know what you learn from your own observations as you try different things.
Normal levels of hematocrit for men range from 41% to 50%. Normal level for women is 36% to 48%. (You will sometimes see different reference ranges). Given what you are describing, I would be sure to review your status with a MPN Specialist. This is complex enough that a regular hematologist may not be able to sort it out as effectively.
I image you already know the diagnostic criteria for ET. Just as a point of reference, here are the diagnostic criteria for PV. Not suggesting that you have PV, just that it helps to understand the spectrum of MPNs and how they present.
Diagnostic criteria for PV as per the 2016 revised World Health Organization (WHO) guidelines include three major criteria and a minor criterion. Diagnosis requires the presence of either all three major criteria or the first two major criteria and the minor criterion. [5]
Major WHO criteria are as follows:
1. Hemoglobin >16.5 g/dL in men and >16 g/dL in women, or hematocrit >49% in men and >48% in women, or red cell mass >25% above mean normal predicted value
2. Bone marrow biopsy showing hypercellularity for age with trilineage growth (panmyelosis) including prominent erythroid, granulocytic, and megakaryocytic proliferation with pleomorphic, mature megakaryocytes (differences in size)
3. Presence of JAK2V617F or JAK2 exon 12 mutation
The minor WHO criterion is as follows:
Serum erythropoietin level below the reference range for normal
Criterion 2 (bone marrow biopsy) may not be required in patients who have sustained absolute erythrocytosis (in men, hemoglobin/hematocrit of >18.5 g/dL/55.5% or in women, >16.5 g/dL/49.5%) if major criterion 3 and the minor criterion are present. However, bone marrow biopsy is the only way to detect initial myelofibrosis, which is present in up to 20% of patients and may predict a more rapid progression to overt myelofibrosis. [5]
Hi HunterThank you for this useful information. I have been trying to understand iron levels and how they affect symptoms. I was diagnosed with PV in September last year and have been having venesections when required. My platelets are around 750 just now and my hematocrit is 40.5. It stayed around 44 following my first round of venesections last year then fell to 40 after a further two venesections in Feb.
I don't know what my iron levels are at present, my haemoglobin is within normal range just now, it was high at diagnosis. I was wondering if you and be iron deficient but haemoglobin within normal ranges??
I have generally been feeling exhausted after venesections, I am better just now. I feel they don't really help with my symptoms.
Interestingly used to donate blood when I was younger but gave up because I felt so awful after.
Also I was in admitted A and E yesterday with chest pain, all tests were fine, and I am currently waiting on a 24 hour heart tracing. I have a history of palpitations/fast heart beat since PV diagnosis but this has got worse recently.
The short answer is yes, you can be iron deficient and have normal HGB. That is the whole point of the venesections. The intent is to induce chronic iron deficiency without inducing anemia. Your body needs iron to make HGB/RBCs.
The KISS explanation is that much of the iron in your body is bound up in the RBCs. As RBCs get cycled out of your body, your body recycles the iron in the old RBCs so new RBCs can be made. Removing whole blood removes the iron in your RBCs. Iron is not easily absorbed through the food you eat, Repeated venesections depletes the iron because you cannot absorb enough iron though diet to replace what is lost to venesections.
Iron deficiency decreases erythrocytosis, reducing our risk of thrombosis with PV. Meeting the HCT target <45% male <42/43% female is a key to managing PV. Like all of our treatment options, venesections have a risk/benefit profile. Iron deficiency without anemia can cause issues like fatigue, loss of concentration, alopecia, and reactive thrombocytosis.
As we make decisions about our PV treatment, we have to weigh the risk/benefit profile of each of our choices. We are reach different in our risk tolerance and in how we respond to each of our options. This is why individualized treatment is so important.
FYI - I also have a history of paroxysmal atrial tachycardia. I had to have a catheter ablation a few years ago to treat it. While the cause is unrelated to the PV, I would note that the increased inflammatory cytokines do not help. Having a cardiovascular condition on top of PV is also an increased risk factor. I also used to have Stage 1 hypertension. My BP normalized when I had the erythrocytosis under control. Hyperviscosity is not a good thing.
Hope you get it all sorted soon. Do please let us know what your learn.
Thanks for your reply. I have been reading around this and slowly beginning to expand my knowledge of PV, but still along way to go with my understandingYour replys are always very helpful and informative.
I do think my cardiac issues are unrelated, but having PV complicates things I guess.
Hi Mauritiu: I hope you get your iron/Hct issues sorted out. There's lots to learn when you're newly diagnosed.
I was interested in your comment that popped up about being admitted to A&E for chest pain. I have also had this occur - 5 admissions in just over the last 3 years, the latest March2022. This time I had tachycardia and heart racing at twice normal. Each time no diagnosis except that it's probably pericarditis/ myocarditis, and no cause found despite extensive tests (cardiac testing, including 24 hour tracing, every blood test you can think of, and this time several infectious diseases panels - all negative). So it's not known if it's PV related, medications related or something else (one cardiologist wondered if it could be a Pegasys side effect, but the first 2 episodes were before I started PEG). A total of 3 cardiologists, 3 GPs and 3 haematologists and still nothing resolved. It knocks me around each time, so I'd like a resolution and hopefully some preventive suggestions. So I'd be interested to hear what you find out. Many thanks for posting. Sharing helps us all.
(dx PV Feb2017; 45 ug Pegasys monthly. Was on daily aspirin, but since the last A&E admission on Rivaroxaban {like Warfarin}, and Sotalol).
HiThank you for your reply and sharing your experience .
Sorry to read you haven't got to the bottom of what is causing your cardiac issues, I do feel I might head this way too. Unless the episode is captured on a recording when it happens I guess its hard to diagnose what is going on . I hope my 24 hour monitoring captures something as my heard does ' little dances' most days.
The A&E consultant suggested it may be PV related but did admit he wasn't sure as his knowledge of PV is limited. He was rather alarmed when I told him during my last episode my heart was at 240 , I have a home monitoring tool. Mine have certainly got worse since diagnosis and more frequent. I have had 4 episodes over Feb/March of prolonged tachycardia lasting half an hour. This episode which took me to A&E was a painful pressure in the middle of my chest but no tachycardia. It gave me a fright as I woke up with it.
As you say it's good to share our experiences with out PV as we all present differently. I will update and share any developments.
I am back to the haematology unit tomorrow for more blood monitoring for my PV, more needles!!
Sorry to hear you both have to contend with the tachycardia on top of a MPN too. I had a catheter ablation where they pass a wire up into your heart through your femoral artery. I was conscious for most of it and got to watch on the monitor. They first detect where the defective node is, then ablate the bad area of the heart. This stopped the higher end tachycardia incidents. I still get occasional minor episodes, but they do not typically go above 110.
I have two types of heart monitors. One is a smart watch that monitors heart rate and can also run a single lead ECG. I also have a Kardia 6-lead device that runs a more sophisticated ECG. I run this ECG when I am having an episode and review with my cardiologist. This is not as good as a full 12 lead ECG, but does provide useful information.
I recently watched this very interesting webinar on how to read a ECG. It is very informative and helps to make the ECG make more sense. It really helps to communicate with your doctors if you have a basic understanding of what they are talking about.
Layne, 44 year old male. I am experiencing the struggle of controlling my HCT and not being too anemic. I have so far avoided going on any extra drugs besides blood thinners. My PV causes my liver to fully clot and stop functioning (Budd Chiari). I miraculously managed to regain function of my liver so less likely to need a transplant.
Over-all I feel pretty lucky to have recovered and that I didn't need a transplant, but now dealing with the extreme fatigue.
Ferritin between 10 - 14 ug/L
Iron between 2 - 5 umol/L
I have only had to have 1 phlebotomy of 250 cc in the last year.
I am supposed to keep my HCT below .45
Have you experienced many side effects, do you have concerns about longer-term side effects?Thanks for posting.
I find the side effects from Besremi to be more tolerable than the side effects of chronic iron deficiency. Also much more tolerable than the side effects of hydroxyurea.
Iron deficiency - fatigue, difficulty concentrating, alopecia, and reactive thrombocytosis PLT +200K.
Hydroxyurea = Oral ulcers, canker sores, thrush, leukoplakia, and constipation.
Of all of these interventions, Besremi (and Pegasys) has worked better and had fewer adverse effects. I also have some cooccurring medical conditions that are a concern. I cannot afford to take chances and do need to maintain control of the erythrocytosis and thrombocytosis.
Inducing iron deficiency is not the best way to do this for me based on my profile, treatment goals, risk tolerance and preferences. I want to manage PV symptoms/risk, reduce risk of MPN progression and maintain a high quality of life. Having my iron levels higher while using Besremi to manage the erythrocytosis is the best way for me to achieve these goals. The intrinsic benefits of Besremi outweigh the risks. We do monitor closely for those risks, but they are not a problem at this point.
Interesting. Perhaps highlighting a case where Besremi is more effective at controlling ET than PV???
My PV “masked PV” whatever you want to call it is odd. Ferritin at 5 yet RBCs increased to upper range limit ever since starting venesections and Hct never quite below 45. It’s almost the opposite of effect of what it’s supposed to do. Half the equation has gone down (MCV) yet other half goes up (RBC) to somewhat equal where I was before I even started venesections. Who knows. I feel pretty good at Hct of 46 but haem is a stickler. If it’s 45.2 she wants a phlebotomy but I’m like nah I’ll wait a couple weeks. I’m her favorite patient. 😆
Your doc is just following the protocol. My doc is like meh, 45.2 is close enough. Wait and see what the Besremi does in a few weeks. That does not mean we ignore HCT, just be a little patient and let the med to its thing. What you describing with iron levels and RBCs makes sense. If you are tolerating the iron deficiency OK then makes sense to continue that plan. If not, there are always other plans.
So in theory once your iron level peaks to your normal level from months of no phlebotomies you can then determine the correct Besremi dose to control hct without the assistance of phlebotomy/iron deficiency correct? If so then if you need to have a periodic phlebotomy while on Besremi, the iron will go back down and you will lose your iron frame of reference for this dosing analysis. Therefore it would seem that over shooting the Besremi dose increase within reason and then backing down the dose once you have hct control is preferred to avoid phlebotomy and the inherent loss of iron frame of reference that would be caused by same. I may be overanalyzing this but I have gone from initial dose of 100 mcg to current dose of 300 mcgs on my 6th dose and perhaps the above analysis is why my doc is not taking a more measured approach on dosage increase. This just occurred to me when I read your informative post. Any thoughts on the concept of over shooting Besremi dose increase to avoid even one phlebotomy for purposes of getting the Besremi dose and iron level balance correct without the potential set back in dose determination that might be caused by phlebotomy and Besremi at the same time?
Your analysis seems spot-on. The Besremi titration protocol is to keep increasing the dose in 50mcg increments until you achieve Complete Hematologic Response. Providing you are tolerating the dose, that make sense. The issue is tolerating the dose you need. While I certainly support the use of Besremi, it has its own side effects to contend with. That also has to be factored in. How you approach the question of Besremi and the continuing use of phlebotomy depends on your treatment goal. My treatment goal is to maintain a complete hematologic response without phlebotomy/iron deficiency. Providing I can tolerate the Besremi dose needed to achieve this, that will continue to be the plan.
I expect that we are going to find that 300mcg is not an uncommon therapeutic dose for many people. The research that lead to approval would certainly seem to suggest this. I think we will also find that some people will do well at a lower dose, while others will need a higher dose. We will also find that what we need will change over time.
Once you achieve the desired hematologic response, you can monitor and see if it stays stable. If the numbers drop off too much, you can always back off on the dose. Do please keep letting us know how you are doing. We will all learn together,
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.