EDIT NOV 28: See larger plot images in reply section below, these are easier to read.
I posted a while ago a plot of allele data from the Conti PV study. I've plotted more of the data from text in the report linked here. I can't find such plots in any public report, I don't know why, they add good visual info. These are my interpretations.
In my opinion the Besremi studies (PROUD and Continuation PV) are among the most detailed and understandable studies for INF in MPN. Plus the only one I know with a simple comparison to HU. Many of the earlier ones for earlier INFs are more difficult for me to follow.
I hope the image not too small, this site limits images to one per post.
This may be part of my presentation to Dr and Insurance Co toward authorizing (paying for) Besremi INF. (this is US insurance stuff, UK and others are very different we've seen here) I have a non-medicare PPO policy. Ins co says we need to show why the new therapy is "beneficial". Interestingly there is no need to compare Pegasys since that is not FDA approved hence not "equivalent". Insurance rep looked for alternatives, expecting to find some. I told her you won't find any, she came back and said you're right.
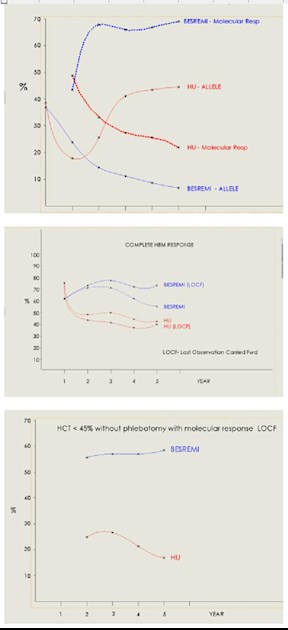
-The top plot has the allele over time for INF (blue) and HU (red) as I posted before. Newly added is molecular response data. Note how widely Besremi and HU diverge in the two measures. Very "beneficial".
-The 2nd plot is Complete Hem Response. It shows two options, one is "Last Observation Carried Fwd". This method provides for patient trial drop outs, and seems controversial in the trade, so I showed as the report also included without that option. All show HU falls below 50% while INF stays above that. Not as striking as the Allele numbers but at 11-22% difference still "beneficial". I don't see any partial Hem response data in the report.
-The 3rd plot is meeting both of the two criteria of HCT<45% and molecular response. This combination is of interest to many MPN patients. This difference is quite clear and beneficial.
There are many quotes from the various reports that support INF being beneficial. I may post a collection I have later. Any other suggestions from our collective collections would be great to have.
It's curious to know whether UK NHS considers Pagasys to be equivalent to Besremi, as above my US Ins co does not require this comparison.
Written by
EPguy
To view profiles and participate in discussions please or .
John Mascarenhas, MD from the Tisch Cancer Institute, Icahn School of Medicine at Mount Sinai speaks about the U.S. FDA Approves BESREMi® (ropeginterferon alfa-2b-njft) as the Only Interferon for Adults With Polycythemia Vera.
Thanks for the link. His discussion of allele reduction tracks well with the 1st plot above, even the cross over of the thin red/blue curves here. It's neat to study that plot as he talked on that.
He also noted the combination studies with INF. I agree that is likely to be in our future.
The Silver MPN Center at Weill Cornell in NYC is a big proponent for interferon and has been for years. Ghaith Abu-Zeinah et al. recently summarized some of their findings in "Normal life expectancy for PV is possible". This was presented at the recent MPN Congress.
I reread my copy of that study "Normal Life". My summary:
Cornell had better MPN care than the general US standard, especially by being early proponents of using the therapies that are now familiar to us. Overall survival (OS) of these patients is superior. Best survival results were from Cornell using INF, see image here, excess deaths started at 12 years not using INF, and non-Cornell patients had the worst outcomes.
One concern I have on this study and their "Long Term INF" study is the high P values in some data sets. These are best under 0.03 for statistical signif, while the upper plot here at 0.33 is 10x that. Maybe I miss something.
It takes close attention to understand this study. SEER are patients getting US national standard of care between 2000 and 2017. WCM RDR data starts in 1974 and are those getting Cornell's (apparently better) standard of care. Some excerpts:
<<PV-SEER patients suffer significantly shorter OS than expected by actuarial statistics>>
<<In contrast, there was no statistically significant difference in OS between PV-WCM and the matched US population... These data point to the success of current standards for
attentive management with aspirin, targeted phlebotomy, and cytoreductive therapy in reducing the early mortality of PV at an academic medical center... Although survival was
indistinguishable between the PV-WCM and the matched US population, the survival curves diverge after about 17 years, suggesting excess late mortality, possibly due to disease progression to MF.,>>
<<in the PV-WCM cohort,...the risk of progression to MF increased over time and affected almost 50% of PV patients after 25 years>>
<<Subgroup analysis of PV-WCM showed that the OS of rIFNα-treated patients (n = 137) was no different than the matched US population (p = 0.33), whereas OS for the remaining non-rIFNα-treated patients was modestly shortened (p = 0.03), with excess death observed ~12 years after diagnosis... PV-WCM patients not treated with rIFNα also survived longer than SEER controls>>
<Both hydroxyurea and rIFNa were associated with improved survival>>
Thanks for the summary. Interesting stuff. I wonder if the WCM numbers being better than SEER is representative at least in part by having an MPN expert involved in care. Am I right to assume that the SEER data may include a significant component of hematologist (i.e., non MPN expert) care for patients?
I agree with your idea. I think Cornell was one of few actual MPN specialists early on. We consider the basics of PLB, HU, asipirn to be obvious treatments where suitable, but I gather in the past these modern basics were less common. I've also heard of chemo options far more toxic than HU that were common in the "old" days. Could be Cornell avoided these.
☺️Thanks all the information. I am in Canada and will have this discussion when needed some day. Not interested in HU if I don’t have to take it. They don’t measure allele burden here so also need to be your best advocate. I have ET so there is always constant thought about progression with every blood test. It is not approved here yet but should be soon. 😀
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.