Buntanetap Is a small molecule that crosses the blood brain barrier and reduces the production of alpha synuclein. No adverse effects were observed in the recent Phase 2 trial: link.springer.com/article/1...
"Buntanetap was safe and well-tolerated in both patient populations. The majority of AEs were attributed to the study procedures (lumbar puncture). There were no clinically significant findings identified in the vital sign measurements or physical examinations. A single AE was noted for a Grade 1 QT prolongation in a patient receiving buntanetap at the confinement visit admission, which resolved and was considered non-clinically significant based on medical history. There was no evidence of treatment-related clinical laboratory testing abnormalities which were considered clinically significant by the investigators. "
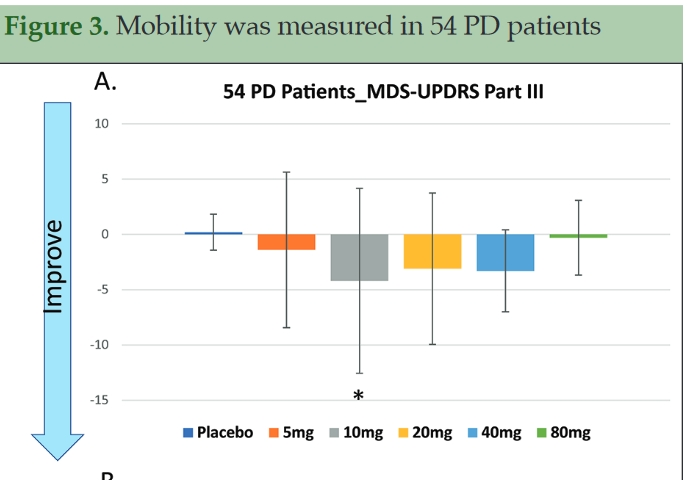
UPDRS part III score improved by 4 points in a remarkably short period of 25 days at the most effective dosage, per image above, from the same link.
The phase 3 trial is testing two different dosage arms, 10 mg and 20 mg, plus placebo, so a participant has a 2/3 chance of receiving active drug. Also, they do not mention lumbar puncture as part of this trial. Usually the intent to use this procedure is stated if it is planned. There are over 30 active sites now recruiting. You can find the locations and their contact information listed here: clinicaltrials.gov/ct2/show...
The inclusion criteria specify Hoehn and Yahr Stage 3 or less. Stage 3: en.wikipedia.org/wiki/Hoehn... “Mild to moderate bilateral disease; some postural instability; physically independent“
The most restrictive of the criteria appear to me to be the requirement for less than or equal to 2 hours of off time daily. Wondering who among us here meets that one. A person wishing to participate in the trial should check the criteria listed at the clinical trials link to see if you qualify.
"So I found this compound that seemed to maybe under certain circumstances, not quite sure, but it could potentially protect nerve cells from dying. And so that was almost 13 years ago I started working on it, and today I know for sure that it protects nerve cells from dying.
It is originally I thought, or what I licensed from the NIH, wasn’t really telling me how it worked. All we knew is that it inhibited one neurotoxic protein that today we know is plaque. As we were working on it, it turned out … And this has nothing to do with us. It’s just the way science has gone … that in the brain of an Alzheimer and Parkinson’s patients, there are a lot of different neurotoxic protein. Not just, say, beta and tau [Alzhemer's], which are the most commonly mentioned, but there’s also alpha synuclein and there’s TDP-43 [the cause of ALS]. These proteins all kill nerve cells. Now, what our drug does is it inhibits them all. How can it work on four totally different proteins? It turns out that these proteins have the same regulatory mechanism, which means that they are made the same way. While they’re four different proteins, their mechanism and how it’s made is identical, and our drug interferes with how they’re made. So because their regulatory mechanism is the same, our drug can act on all four, and it does inhibit neurotoxic proteins. And by doing so, it protects nerve cells from dying."
“cells. Now, what our drug does is it inhibits them all. How can it work on four totally different proteins? It turns out that these proteins have the same regulatory mechanism, which means that they are made the same way. While they’re four different proteins, their mechanism and how it’s made is identical, and our drug interferes with how they’re made. So because their regulatory mechanism is the same, our drug can act on all four, and it does inhibit neurotoxic proteins. And by doing so, it protects nerve cells from dying."
At which site are you participating? I'm going to Kansas City. I just made my second visit and received my first dose of either Buntanetap or the placebo last Thursday.
Ah. One way to go about that would be to self administer UPDRS part III before, and then after a month of treatment and see if you get a few points of improvement.
They told me that I MIGHT be able to find out whether I received the placebo after the trial has been fully completed and that I MIGHT then get access to the real thing if it proves to be effective, but that has not yet been determined. My research doctor said they advocate for such action to encourage future participation in trials and because it's ethically challenging to pull a drug away from participants (regardless of whether they initially received the placebo) if the actual drug proves to be beneficial.
It would have given me pause if I had read it before starting the trial, but I am already more than half way through the trial and haven't felt or experienced any negative side effects so I will see it through to the end. If the folks at Annovis Bio have a propensity for exaggerating, it's certainly disconcerting.
We will likely have an open label study next year. That depends on several things, one of them being the blessing of the FDA for us to move ahead to longer trials. If we are able to conduct an open label study, then those who participated in our current trials may be eligible.
These results are not actually recent. When last year they were first announced, the share price of Annovis rocketed. Later normality was restored. Also Buntanetap is not new - it was previously called ANVS-401 or Posiphen.
I dont want to be negative as it’s not my nature but there seem to be other views about Annovis’s research disclosures. If any of the matters in the following article are true (especially relating to the allegation of exaggeration), a dampener is placed on what sounds like an exciting prospect.
What I find most intriguing about this trial is the claim that the proteins associated with ALZ, ALS, and PD all have the “same regulatory mechanism.” This is reason to hope that as treatments for ALZ are found, they could likely apply to PD and ALZ has far more funding and interest than PD.
I am not going to take on the criticism of buntanetap in the treatment of Alzheimer's because that is not relevant here.
Regarding Parkinson's, that writer is concerned the good phase 2 results are a result of acetylcholinesterase inhibitor properties possessed by a drug that is the enantiomer (mirror image) of buntanetap, known as phenserine. Annovis is insistent that the mode of action is quite different, as displayed in my above comment. It is commonplace for enantiomers to have quite different properties in biology - this why we take levodopa and not dextrodopa. However, it is not necessary to rely upon general principles, or to take Annovis’ word for it. We need merely look up the use of acetylcholinesterase inhibitors in the treatment of Parkinson's:
ncbi.nlm.nih.gov/pmc/articl... (2022) “Dopamine based therapies are used for the treatment of motor symptoms. Non-motor symptoms are treated with other medications such as … acetylcholinesterase inhibitors (dementia),”
link.springer.com/article/1... (2020) “Cognitive dysfunction is common in Parkinson’s disease (PD)... It is associated primarily with pathologic involvement of basal forebrain cholinergic and prefrontal dopaminergic systems… Dopaminergic medications and deep brain stimulation help motor dysfunction, but may have potential cognitive side effects. Central acetylcholinesterase inhibitors, and possibly memantine, provide modest and temporary symptomatic relief for dementia”
Acetylcholinesterase inhibitors are NOT used as a remedy for Parkinson's Disease motor impairment. This is precisely where buntanetap shines, based on the UPDRS part III result.
I am scheduled for a screening 4/4 but should I be less enthused now?
Maybe this explains claims of exaggeration.
"Conflict of interest statement
Cheng Fang, Eve Damiano and Maria Maccecchini are employed by Annovis Bio. Priscilla Hernandez and Kore Liow received funding from Annovis Bio for the conduct of the clinical trial, Henrik Zetterberg and Kaj Blennow received funding from Annovis Bio for biomarker analysis and Michael Chen and David Feng received funding from Annovis Bio for statistical analysis."
"Based on the current enrollment, the Company anticipates having a sufficient number of patients who have received two months of therapy to conduct an interim analysis in the second quarter of 2023. The purpose of the interim analysis is to determine if the Company's original estimates for patient enrollment in the Phase 3 trial (150 patients per arm) will be sufficient to observe a statistically significant treatment effect in both scales between the active arms and the control arm of the study after six months of treatment.
More specifically, the interim analysis could confirm that 150 patients is the optimal number, or it could inform that less patients are needed (the efficacy is better than expected) or that more patients are needed (the efficacy is less than expected). The boundaries of the extent to which we will decrease or increase the number of patients is +/- 25% or between 112 and 200 patients per arm."
I wonder why higher dose lesser effect, at 80mg almost no effect. And the results only 25 days, does that higher dose OR longer period the effect will be gone? Hopefully not.
Buntanetap reduces production of alpha synuclein. Both excess and defectively folded alpha synuclein can cause Parkinson’s. Nonetheless some alpha synuclein is necessary - Mice that lack α-synuclein gene demonstrate impairments of working memory and spatial learning.
Really? Why have Annovis not offered this explanation?
The study you cite referenced cognitive outcomes. But the Buntanetap graphic was UPDRS. The study you link to states that mice with a-syn "knocked out" did not experience adverse motor responses
"On the first stage of the work locomotor abilities of experimental animals were estimated. The α-KO mice showed a slightly decreased motion activity. However, at the same time statistically significant difference in force and stamina was not shown. Moreover, on average the rates were even better. Previous research had not revealed any locomotor disorders in the α-KO group as well [2], [34]."
My emphasis.
Even as a hypothesis, rather than established fact, does it work? How does it explain 80 mg being MORE effective than 40mg? Or placebo MORE effective than 10mg?
We have a quiz show called "QI" in the UK where it is possible to play a kind of joker card for bonus points if the correct answer to the question is "Nobody knows"
Total updrs results graphic for buntanetap (source Annovis)
The Phase 2 study also turned in good results for the WAIS - COG, in other words good results for both non-motor and motor symptoms. so the animal study I cited is relevant.
Also, Maria has made it quite clear that high doses of Buntanetap do not work for Parkinson's
This is the guy who cannot believe that buntanetap might behave differently than its mirror image. As I said in my reply to lyricist, this is why we take levodopa and not dextrodopa. I'm going to have to stick with that reply because right now I do not have the time or energy to dig into the linked post further.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.