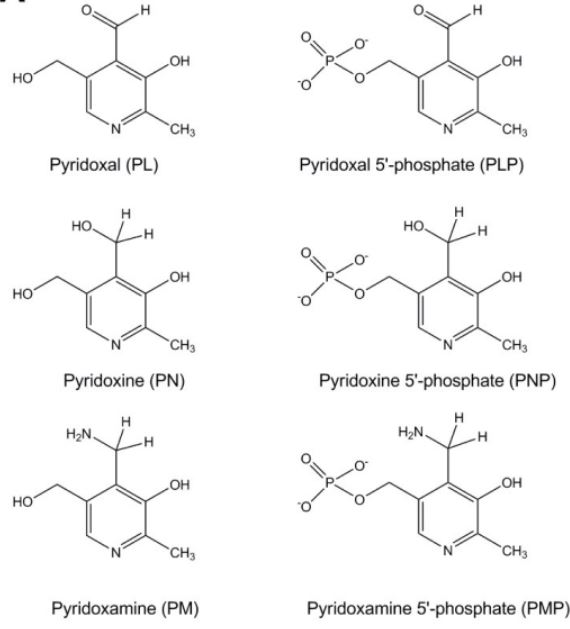
Different forms of vitamin B-6. Credit: openi.nlm.nih.gov/detailedr....
Carbidopa uses up vitamin B6. Vitamin B6 is essential for all manner of biochemical wizardry, so it is not something we want to be short of. Vitamin B6 and carbidopa bind together and inactivate each other, so they cannot be taken at the same time. One way around this problem is to give up carbidopa entirely, which was the reason for the Hinz protocol. Another solution is to simply take them a couple of hours apart or separate by a meal.
It is essential to avoid pyridoxine, the version of vitamin B6 that causes toxicity:
sciencedirect.com/science/a...
The vitamin B6 paradox: Supplementation with high concentrations of pyridoxine leads to decreased vitamin B6 function
"Vitamin B6 is a water-soluble vitamin that functions as a coenzyme in many reactions involved in amino acid, carbohydrates and lipid metabolism. Since 2014, > 50 cases of sensory neuronal pain due to vitamin B6 supplementation were reported. Up to now, the mechanism of this toxicity is enigmatic and the contribution of the various B6 vitamers to this toxicity is largely unknown.
"In the present study, the neurotoxicity of the different forms of vitamin B6 is tested on SHSY5Y [a human derived neural cell line] and CaCo-2 cells. Cells were exposed to pyridoxine, pyridoxamine, pyridoxal, pyridoxal-5-phosphate or pyridoxamine-5-phosphate for 24 h, after which cell viability was measured ... Pyridoxine induced cell death in a concentration-dependent way in SHSY5Y cells. The other vitamers did not affect cell viability. .... Moreover, both pyridoxal-5-phosphate dependent enzymes were inhibited by pyridoxine. In conclusion, the present study indicates that the neuropathy observed after taking a relatively high dose of vitamin B6 supplements is due to pyridoxine. The inactive form pyridoxine competitively inhibits the active pyridoxal-5-phosphate. Consequently, symptoms of vitamin B6 supplementation are similar to those of vitamin B6 deficiency."
So the moral of this story is if you are supplementing vitamin B6, do not take it as pyridoxine, which is frequently what you get in multivitamins. Take pyridoxal-5-phosphate (P5P) instead. It is readily available as a supplement.
Report regarding human neuropathy due to consumption of high doses of pyridoxine:
pubmed.ncbi.nlm.nih.gov/250...
Pyridoxine-induced sensory ataxic neuronopathy and neuropathy: revisited
"High dose pyridoxine is neurotoxic... Three patients, aged 80, 83 and 83 years old, presented with sensory ataxia for 3-8 months. Examination showed signs of polyneuropathy and sensory ataxia. Six hundred milligrams of pyridoxine was consumed each day for 3-10 years, in the form of vitamin B1-6-12 combination tablet. [Neurobion, manufactured by Merck, Ltd., which contained vitamin B6, as pyridoxine, 200 mg]
Investigations for other causes of neuropathy were unremarkable. Blood levels of vitamin B6 were markedly elevated at 104.6, 81.4 and 66.9 times of upper normal limits.[These were measurements of the non-toxic P5P, not the toxic pyridoxine. Unfortunate that they did not measure those levels] Electrodiagnostic tests showed symmetric axonal sensory polyneuropathy in two patients. Two years after vitamin discontinuation, all patients showed no significant improvement in the neuropathy and gait. In conclusion, consumption of high dose pyridoxine can cause sensory neuronopathy and axonal sensorimotor polyneuropathy, leading to sensory ataxia which may not be reversible. "
Update 2023-12-10:
B2 deficiency can also cause high levels of pyridoxine and consequent toxicity. See: healthunlocked.com/cure-par...
For Parkinson's patients taking levodopa medication, failure to supplement B6 can be disastrous as set forth here: healthunlocked.com/cure-par...

")