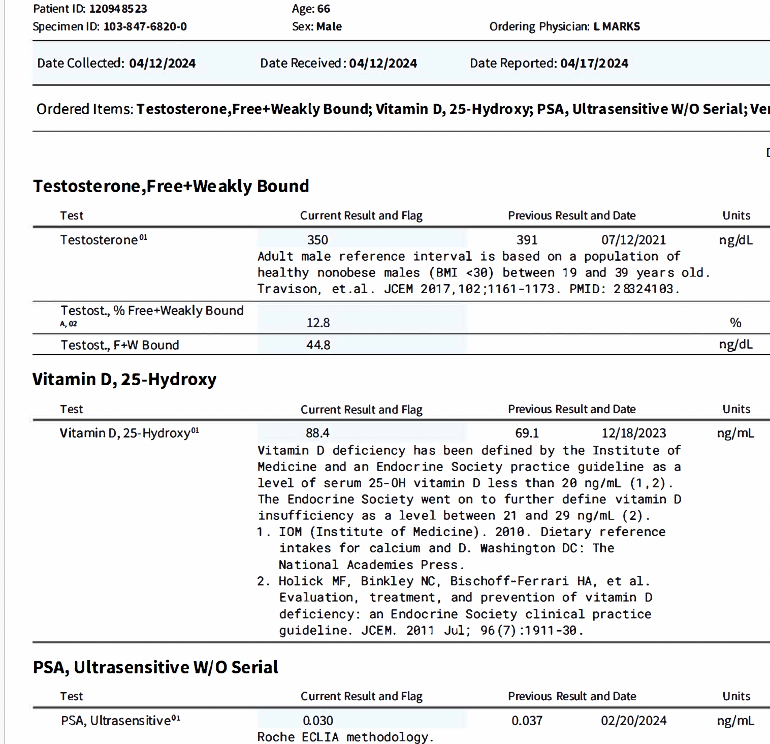
A prostate cancer brother who ask me to return to HU (blame him ;), recently asked me about my T levels. Mid-day today I texted him the results which came in while on a coffee break following my morning of most excellent spring skiing. He texted back what I have used for the topic of this post.
Yes, I find usPSA useful post RP and when not on ADT (I was on bicalutamide one year only ending five years ago). As I frequently share, six years ago, March 2018, I had salvage extended pelvic lymph node surgery following amazing imaging in Europe, at usPSA 0.11. Despite six pelvic nodes being confirmed cancerous, my post ePLND nadir was <0.010, which held for two years. It slowly rose through 0.01X and 0.02X ranges, and has has been very low stable 0.03X range since June 2021. I remain grateful beyond words.
All the best to all of us fighting this beast!
Written by
NanoMRI
To view profiles and participate in discussions please or .
Excellent report, congratulations! If you are not aware of, they did a test in Germany* comparing 4 different analysers. They had a number of blood draws, divided them in four vials and sent them to 4 hospitals for routine analysis on 4 different sets of kit. They then got every set of four reports, calculated the average value and compared each report against the average. Two analysers scored on the high side, the remaining two on the low one. Roche was the highest, Abbott the second runner for the high side. Don't recall the two low ones.
Additional info:
(*) Remember that it was in Germany, but now that I searched again the authors are in Italy - strange
"We included in this study 4 most recent generation MSs (Measuring Systems):
Another strange thing in the above mentioned paper is that the comparison is made against the "All methods median μg/L" which, for an (even) group of 4, equals the average of the middle two and not the average of all four, as I thought. Doing this, the two remaining (min and max) are treated as outliers and discarded. Not sure if this is justified or adopted just to render data proccessing simpler.
The 'other' numbers and variances that IMO warrant more attention are the annual death rate and the number of men on ADT (despite all the 'science' and 'advancements' they are not declining). I do graph my usPSA results - very revealing. Retrospectively, I graphed the fluctuating results from my years of PSA screening - prior to diagnosis. That graph clearly shows a steady rise of the lows. Unfortunately, my doc and I focused on the drops of the highs. We were falsely dismissive of the very thing we were screening for. Cancer.
Great perspective and great results. As a man on adt at 53 its been a tough road.
While some consider usPSA nothing more than an "anxiety stir" I can see how this has paid off for you. With a T <10, I can't say I'm a fan of adt and all of the metabolic dysfunction it causes.
And as a guy who went through surgery, recurrence, radiation and hormone therapy all within 12 months, I couldn't agree more that the goal should be early detection and avoiding adt for as long as possible. The day we start adt is the day we start the clock to castrate-resistance.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.