This pathology report should make you somewhat happy because it has many good prognostic factors. (The best thing would have been him having NO Pca.)
(1) Your husband's PCa is plain adenocarcinoma which means a regular, garden variety type of Pca ..which occurs in close to 92% of people. Fortunately, he does not seem to have ductal, small cell or neuro-endocrine types which are more aggressive.
(2) Another good news is that his Gleason Grade is low. i.e. 3+4=7 only. This indicates that his cancer cells are less virulent and thus less likely to metastasize. These cells are very less deformed and distorted so they are less mean and less aggressive.
(3) Again, not having seminal vesicle invasion, lymph node invasion, vascular invasion , having negative surgical margins ..are all good signs.
(4) The icing on the cake is low PSA (0.03 )
If you put all these factors together and take a composite picture, he is likely to have many many years of progression free and overall cancer specific survival.
Dublin, you probably already know that 3+4=7 means that when pathologist looked his cancer slide under the microscope, he/she saw most of the cells as "non cancerous" (thus gave number 3) but then he/she saw some cells as mildly cancerous (thus comes number 4) So basically his cancer cells are very mild type and very less in number...good thing indeed !
There are some "not so good" elements in your husband's pathology that LearnAll was kind enough to overlook.
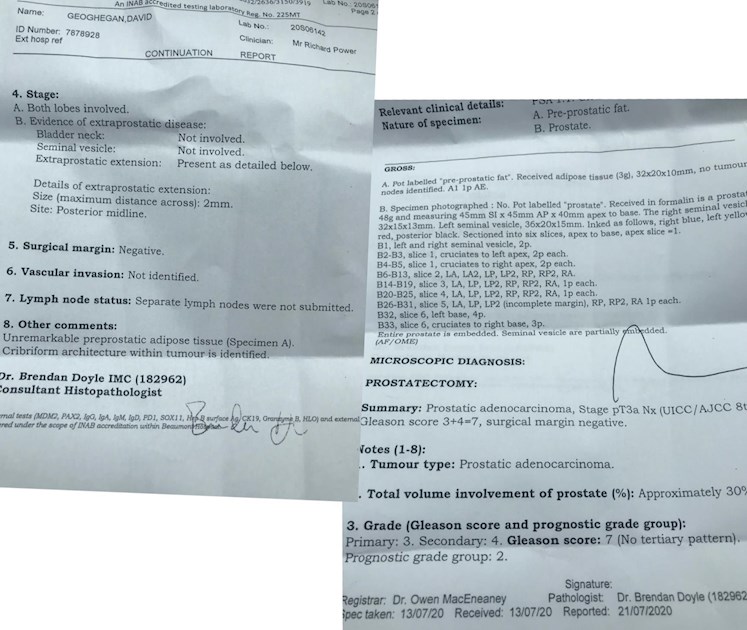
"pT3a Nx" it writes.
a) pT3a relates to extraprostatic extension, i.e. not fully contained within the prostate.
b) Nx means that there were no lymph nodes examined, probably none dissected, so it is not known what happens in this domain.
c) PSA 0.03, is borderline. I would recommend monthly PSA followups.
Thanks Justfor..that is totally just...I still believe that the good features override little bad ones. As for monthly PSA, I do it myself...so all for it. BTW, My Gleason Grade is also 3+4=7. WE are all Irish, because we are " potato eaters" I am not from Ireland but I am certainly a "potato eater" My Doctor once said " If you have prostate cancer, you can safely eat any food which comes from under the soil". BTW, thank you for pointing out the lacunas.
"You and I we’ve been through this, and this is not our fate
So let us not speak falsely now the hour is getting late"
From Bob Dylan's "All along the watchtower", a song from my youth.
As a gesture of courtesy LearnAll, I leave the talent distribution to you (joker, thief, riders). I will only keep open the "princes'", in case J-O-H-N casts for the role (smiling face here).
• in reply to
“Two riders approaching” said the joker to the thief
So that's a fair first PSA, and a fair pathology report. The upsides are no positive margins, and a pretty low Gleason score. The downsides are the large tumor, the cribriform pattern and the focal extraprostatic extenson (2 mm- which may be insignificant). There is nothing to do now but monitor PSA. If it rises steadily or hits 0.1, salvage radiation may be necessary. A recent study proved there is no benefit to getting salvage radiation any earlier.
Of course I don't mind. Just remember that most guys on this site are coming from a place of having advanced PC, which does not apply to you. Their advice may be alarming, wrong, or irrelevant.
Yes...I welcome you to stay with us. Tall Allen himself is non metastatic and he has been staying here since beginning of time and will stay here till end of the World.
I just read that 70% of people who were not diagnosed metastatic were found to have bone mets in post mortem/autopsy findings.
References:: The bone microenvironment in metastasis :what is special about bone By Bussard KM
Overview of diagnosis and management of Metastatic disease to bone. By Yu HH 2012.
"If it rises steadily or hits 1.0, salvage radiation may be necessary. A recent study proved there is no benefit to getting salvage radiation any earlier."
Which study do you refer to? This is very interesting.
None of the links indicates a PSA of 1. Did you find the link?
"
"Early salvage" radiation (eSRT) was defined variously as treatment when PSA ≥ 0.1ng/ml or 3 consecutive rises (RADICALS-RT), PSA≥0.2 ng/ml and rising (GETUG-AFU-17), or PSA≥0.2 ng/ml (RAVES).
I assume the 1.0 is a typo and should read 0.1 instead. I did not have the intention to spot a typo, so I did not reply to that.
However, 0.1 is rather low, the usual range is 0.2 to 0.5 to start with salvage radiation. The statistics say, 0.2 is better than 0.5. prostatecancer.news/2016/08...
The criterion for receiving early SRT was either 3 consecutive uPSA rises or PSA≥ 0.1ng/ml. Of course, some patients will have had persistent PSA, which was already greater than 0.1, and some patients may have delayed SRT for some reason. That increases the median.
Detectability is only in relation to the sensitivity of the test used. 0.03 is detectable on an ultrasensitive PSA test. 0.1 is detectable on a conventional PSA test.
I get that. So is the implication that anything over 0.00... on an ultrasensitive test is worrisome? I don’t mean to be difficult, but I thought that you advised not monitoring seemingly minute changes with an ultrasensive PSA test.
There are a number of retrospective studies trying to correlate prognosis with the first PSA value (first PSA is usually taken at 3 months after RP, so there is some ambiguity if the same values apply to 4-6 weeks post RP). The cut-off numbers are a bit blurred. Some state less than 0.03 (others include 0.03 by stating less or equal to 0.03) signals a good prognosis. The consensus for a bad prognosis is at 0.06 and above. Consequently, 0.04 and 0.05 lay in the grey area between the mentioned two.
In APC such small values are the result of ADT. Post RP, on the other hand, they can represent normal (benin) PSA secretion either from tissue left back or from a small number of other organs that also do so. Hence, an absolute zero is not a prerequisite for an absence of malignancy. The acid test is the afterwards PSA rise which is indicative of the proliferation of cancerous cells.
No. What RADICALS-RT proved was that three consecutive rises or a PSA of 0.1 is a good signal that salvage radiation is necessary.
" I thought that you advised not monitoring seemingly minute changes with an ultrasensive PSA test."
It depends on the situation. For someone who has had a prostatectomy, an ultrasensitive PSA can catch an early signal to get possibly curative salvage radiation. For someone who has had primary RT, has had salvage radiation already, or has had metastases, an ultrasensitive test has no prognostic validity and will only cause anxiety.
For clarification: He should be getting an ultrasensitive PSA test at his next bloods.
A PSMA PET scan is entirely different thing. It is probably not available where you are, and even if it were, it will not show anything at his low PSA. (PSMA PET detection is highly dependent on PSA). It is not dangerous, just useless for him.
If the PSA doesn't change you will get a month's worth of pause.
If it changes, you will have to wait until it is more than 0.1 (any doc/rock you will "try to turn over" will say 0.2 at least- most will try to dissuade you altogether).
PSMA PET/CT is both expensive and also the patient receives some radiation.
I do not believe that the healthcare system in ROI will approve such a PET/CT for PSA less than 2 (yes, two i.e. 2,0 - not 0,2) so you will have to pay out of pocket. Prices in central Europe range from 1500 to 2000 Euros.
Regarding radiation, is something like ~ 3 CT or 5 transatlantic flights (my own estimates).
Bottom line: Stay calm, if you want us to remain friends (smiling friendly face here).
Nope? I’m on the ultra sensitive test . I’m testing <0.014 and this is considered undetectable. A biochemical recurrence is stated as O.200 or greater .
Joker/Thief (pending) to princes:
0.1 is the lowest PSA for salvage RT consideration.
Any reason why they didn't take any lymph nodes? Now you miss that in the staging (pT3A Nx). If the PSA is undetectable at 9 and 12 months there is good chance that PC is over for you. Good luck!
Your husband is PT3 (cancer has escaped the prostate) which is not as good as pT2 (cancer contained in prostate). He needs monthly PSA monitoring. Since the cancer has escaped the prostate and no lymph nodes were dissected there is no way to know if the cancer is still in the prostate bed or worse case in the lymph nodes. Therefore monthly monitoring is need to see if PSA rises. If it does, radiation and hormones will be required. This will hopefully kill any remaining cancer cells in the prostate bed. Very worst case cancer has gotten into lymph nodes and already metastasized. Hopefully that won’t be the case. To be quite honest 0.03 is not the greatest initial PSA reading. I have a feeling he will need radiation and hormones in his future.
I am really surprised that the surgeon didn’t remove lymph nodes. Usually if you have extracapsular extension lymph nodes are removed. May I ask who your surgeon was.
The reason I ask is my surgeon did not take any lymph nodes during my surgery. His feeling was that you will know if the cancer is still present by a rise in PSA. So why bother.
It is case specific why the surgeon didn’t take the nodes. My Mo recommended no radiation to my lymph nodes due to only two out of seven being lit up on scans . It was the right decision . I was never a candidate for surgery .....I think that you both can live healthy love each and and have many years together . Remember we are not doctors here . Follow professionals .. 😷✌️
You have benefited from good advice from the wiser members of this forum. Words like "aggressive" are subjective and should be taken with a "grain of salt." What is important is the behavior of the tumor. That pathology report is one piece of data and these generally read more grim. You cannot change the pathology report. You and he can do everything possible to promote good health in terms of attitude, exercise and eating. And the PCa will tell its story through the PSA testing. In the hands of the Gods now. Go n-éirí leat!
I would recommend you get a second pathology opinion from the well known pathologist Dr Johnathan Epstein at Johns Hopkins. He is the best in the business.
We are in Dublin so I’ll straight away start to look for the best here. Although we were told we had the best, when we chose Dr Richard Power, by so many people pre RALP . I question this now.
I do not see the percent of cancer that is Gleason 3.
No Lymph nodes taken during surgery for examination so no further clue on if the microscopic extra-prostatic extension (EPE) is significant. Also, was the EPE Gleason 3 or Gleason 4?? Can the Pathologist tell??
Your husband's age??
30% of the prostate gland is cancer involved.
I do not see how much (%) of the cancer is Gleason 3 & how much is Gleason 4.
In the past some Docs would give Adjunctive Radiation Treatment (ART) for EPE but from what I could find not so much today. Today many seem to wait for a BioChemical Re-occurrence (BCR) which is frequently defined as when the PSA goes to 0.1 or more. At that time the Radiation Treatment is called Salvage Radiation Treatment (SRT).
Lack of cancer in the seminal vesicles is good news as many authorities feel this is how cancer gets into the bloodstream as the seminal vesicles are quite vascular.
My question is with microscopic-EPE, no lymph nodes to examine and your Doc saying the cancer is aggressive. Given these, would your Doc consider ART or would your Doc wait and give SRT if/when a BCR is detected??
Also, are you seeing a Medical Oncologist (MO) or just the Urologist??? If only the Urologist you might want to get another opinion from a MO. If the MO confirms the Urologist's path of treatment you can be assured .... if not there are decisions to be made.
Prostate Cancer is like Breast Cancer, once you have had it you are on watch for a possible re-occurrence for the rest of your life. Both of these can come back years and rarely even decades later. I have a friend age 46 who just had surgery. So this can affect relatively young people. The good news is your husband's cancer appears to have been caught relatively early. He may very well be cured but still needs to be on watch. My cancer was Gleason 3 (85%) + 4 (15%) = 7 with 20% of the gland affected, 2x microscopic positive surgical margins, 2x microscopic EPE's and was negative for cancer in 11 lymph nodes that were taken during surgery. The Pathologist was unable to determine if the Cancer at the positive surgical margins & at the EPE's was Gleason 3 or Gleason 4. My Urologist said no more treatment at this time. My MO (an internationally recognized researcher) said ART is recommended, which I completed ..... so opinions can differ. Your husband's Pathology results are a bit different than mine and your husband is younger (I was 67 at diagnosis) so with differing Pathology your husband may in fact require no additional treatment at this time but I suggest you consult with an MO to be sure.
In either case, your husband should get all the recommended PSA tests and stay on watch.
I was 53 and much worse off than he is . I think he’s going to live for decades . This pc stays with us in some form until the end . Many here have survived. With it for decades . Just try to have him live and eat healthy . God bless your family !🙏🌵
Agreed. My uro and Mo differed in my treatment plan , I went with the mo pc specialist over the uro .. Glad I did . The uro said Id be dead in 36 months . I’m at 57 months now with no signs of pc .
A comment from downunder. In general his histo looks favourable with low risk Gleason score and I wouldnt normally call that aggressive. Yes he has positve surgical margins but that is relatively common, post RP. Two options, either be heroic and get a PSMA PET scan and treat any PSMA avid lesions with Lu177 at this early stagee (sorry it will cost you) or do nothing apart from PSA tests (3mo) and have radiation to the prostate bed (salvage, so called) when PSA levels get over 0.2ng/ml. In both cases, enjoy living.
Ride this good Psa as long as you can . I’ve been clear almost five years now when my uro told me I’d be long gone by now .. love of you and family are the best reasons in this world to stick this out ...he possibly could be done with pc for good . 🙏😷. He’s got lots of love . This is a good life .❤️
His age is important because the size of his prostate is the one of a 70 y.o.
Did you met other doctors than the surgeon.
Did they explained the mortality factors and the morbidity factors.
I had my biopsies on Jan 29 2020, the diagnostic on March 3rd 2020 where the multiple choices were presented to me and then the ADT was started on April 4th and the VMAT RT was started on June 8th 2020 and finished on July 07th 2020.
I am a G4+7 Grade 3 Intermediary unfavorable risk.
Your husband is lucky to be a G3+4 Grade 2.
My PSA pre-biopsies was 13.6 then went up to 20.4 and after RXs went down to 0.18.
Do you know if the surgeon did a nerves sparring? If not, your husband wont be able to have erection. Problem that I will not have when my ADT finishes.
Ok so I get that, which I wouldn’t have until you said. He’s having another blood test done in 2 wks but in the mean time what scan should I be looking To arrange.
Only scan He’s had is prostate mri. That’s how it’s done here but I’ll do what I have to to turn over any stones.
As I can see, if he had the option of RO, the RX will have covered the EPE margin and he would not have to go trough the whole secondary effects due to a prostatectomy.
That is the reason for having the WHOLE team to help for the decision.
You really have raised my awareness in them and I will ask the questions. His bloods will be done again in 2 wks and I will push psma scan from there and raise all these details with mo. I now need to find a good mo. Far as a think the urologist surgeon is not being specific and looking at details in pathology. He’s waiting on growth for then recommending further treatment.
According to this all-round article on PSMA, as a diagnostic or a therapeutic means, it is the exact opposite:
"It is worth noting that the PSMA protein contributes to the survival of the cancer, and just the PSMA ligand that attaches to it has some activity in delaying progression, even without a radioactive component (similar to the way an anti-androgen attaches to the androgen receptor, delaying progression)".
There is always secondary cancer risks related to all radiation exposure!
But, of course, the benefits of scans outweigh the risk, when the doctors suggest scan. Note that PSMA PET/CT scans do not show anything useful until PSA is 0.2 or higher so it is often not applicable after RP since SRT is often initiated at lower PSA.
Have you seen the movie entitled Catch 22? This 0.2 magic number is the "I don't want to know because if I do I will have to do something about it" doctor's catch 22 refuge. Unfortunately, for the patient that is, mother nature is still functioning in an analog maner with no intention to switching to binaries 0 or 1 for the foreseeable future.
Most patients undergo salvage RT without local imaging since if you wait until mets are detectable it is too late to treat. You shoot more or less blind.
The same paper goes a bit more in depth by publishing probability coefficients from more granular data. Found in tables 4 and onward they are calculated from a subgroup of cases that had available the necessary data. One important independent variable is PSA doubling time (PSADT). You will get a grasp of your husband's PSADT after having 3 tests, although I wish him and you to learn the actual value after many-many-many years.
Doing some arbitrary guess-work on the latter (don't ask me-won't tell you) I see the following probabilities vs PSA:
There are a lot of different scans, some just READ the organs after an injection of radio-active solutions(PET-Scan, Bone Scan) and others that send X-Ray (Cat-Scan). The PSMA Scan is unknow to me. But I think it is a mix of the 2.
PSMA PET-CT Accurately Detects Prostate Cancer Spread, Trial Shows
May 11, 2020, by NCI Staff
Images from a Ga-68 PSMA PET-CT in a man with prostate cancer shows tumors in lymph nodes in the chest and abdomen.
Credit: Adapted from Int J Mol Sci. July 2013. doi: 10.3390/ijms140713842. CC BY 3.0.
For some men with prostate cancer, results from a large clinical trial suggest that there may be a more effective imaging approach to detect the spread of their cancer to other parts of the body than the approach that is most commonly used.
Conducted in Australia, the trial included men diagnosed with localized prostate cancer that was thought to be at high risk of spreading beyond the prostate. In the study, an imaging method known as PSMA PET-CT was substantially more likely to detect metastatic tumors in these men than the standard imaging approach used in many countries, which involves a CT scan and a bone scan.
Use of PSMA PET-CT also was more likely than the standard approach to change the strategy doctors used to treat the cancer, the trial’s lead investigator, Michael Hofman, a professor of Nuclear Medicine at the Peter MacCallum Cancer Centre in Melbourne, and his colleagues reported March 22 in The Lancet.
The trial was not designed to show whether using PSMA PET-CT improved clinical outcomes like how long patients lived. But the results, Dr. Hofman said, build on evidence from other studies and current clinical practice in countries like Australia and Germany that suggest PSMA PET-CT is more likely to detect metastases than the conventional approach.
“For a diagnostic test like this, accuracy is the most important thing. You want an accurate test,” Dr. Hofman said. Because, in this patient population, he noted, the presence of metastases should affect how men are treated.
If the cancer has spread beyond the prostate at the time of diagnosis, treating the primary tumor in the prostate with surgery or radiation on their own “is a futile exercise,” Dr. Hofman said. Knowing early after diagnosis whether the cancer has already spread “is key to better optimizing the treatment for these men.”
The Food and Drug Administration (FDA) hasn’t approved any PSMA-targeted imaging agents, so PSMA PET-CT isn’t available in the United States outside of clinical studies, explained Lalitha Shankar, M.D., Ph.D., of the Cancer Imaging Program in NCI’s Division of Cancer Treatment and Diagnosis.
Several PSMA-targeted imaging agents are being studied, Dr. Shankar said, and “they are all quite promising.” But further studies are still needed, she continued. In particular, additional clinical trials that carefully examine how these imaging approaches “affect patient management” would be helpful, she said. “We also need to see whether there is an impact on outcomes.”
A Different Way to Detect Metastases
Most men diagnosed with prostate cancer have localized disease, meaning the cancer appears to be confined to the prostate gland. However, certain factors have been linked to a higher risk of the cancer eventually spreading (or having already spread).
Currently, in the United States and many other countries, most men diagnosed with high-risk localized prostate cancer undergo additional testing to see if there is evidence of metastatic cancer. For many years, that has been done with a conventional CT scan (which uses a form of x-rays) and a bone scan (a type of nuclear imaging test), the latter because prostate cancer often spreads to the bones.
But both imaging technologies have limitations. Neither is particularly good at finding individual prostate cancer cells, and thus can miss very small tumors. And bone scans can detect bone damage or abnormalities that were caused by something other than cancer (e.g., arthritis), resulting in “false-positive” findings that can lead to unnecessary additional testing.
So, researchers have been developing and testing other imaging agents that can find prostate cancer cells specifically in the body, Dr. Shankar explained.
As their name implies, PET-CT scans combine a CT scan with a PET scan, another type of nuclear imaging test that requires patients to receive intravenous injections of a radioactive “tracer” that can be detected on the scan.
In a PSMA PET-CT, the tracer used for the PET scan includes a molecule that specifically binds to the PSMA protein, which is often found in large amounts on prostate cancer cells. That molecule is linked to a radioactive compound, or radioisotope. The radioisotope used in the Australian trial is called gallium-68 (Ga-68).
PSMA-targeted tracers that use other radioisotopes are also being widely studied, explained Martin Pomper, M.D., Ph.D., director of Nuclear Medicine and Molecular Imaging at the Johns Hopkins School of Medicine. Smaller studies have strongly suggested that PSMA PET-CT is better at detecting metastases in men with localized prostate cancer, Dr. Pomper said, so more definitive answers from larger studies have been anxiously awaited.
Greater Accuracy and Changing Treatment
Approximately 300 men were enrolled in the Australian trial, all with newly diagnosed localized prostate cancer (based on a prostate biopsy), and all were considered to have high-risk disease. For all men in the trial, the planned treatment was either surgery (prostatectomy) or radiation therapy to the prostate only.
Half the men were randomly assigned to initially undergo a CT and bone scan, and the other half to PSMA PET-CT.
Based on the imaging, PSMA PET-CT was 27% more accurate than the standard approach at detecting any metastases (92% versus 65%). Accuracy was determined by combining the scans’ sensitivity and specificity, measures that show a test’s ability to correctly identify when disease is present and not present.
PSMA PET-CT was more accurate for both metastases found in lymph nodes in the pelvis and in more distant parts of the body, including bone. Radiation exposure was also substantially lower with PSMA PET-CT than with the conventional approach.
The trial investigators also tracked how imaging results influenced clinicians’ treatment choices. Based on imaging findings, the initial treatment plan was changed for 15% of men who underwent conventional imaging compared with 28% of men who underwent PSMA PET-CT.
Another key finding, Dr. Hofman noted, was that PSMA PET-CT was much less likely to produce inconclusive, or equivocal, results (7% versus 23%).
That’s important, he continued, “because if you have a scan with equivocal findings, it often leads to more scans or biopsies or other tests.”
The Future of PSMA PET-CT
“This is a solid study and reflects the real-world experience” with PSMA PET-CT in other countries, Dr. Pomper said. Because there are several PSMA-targeted tracers, a next step will be to have them approved for use in the United States outside of clinical trials, he added.
He predicted that, eventually, the different PSMA tracers will be tested head to head.
The Australian trial adds to a growing body of research on improving the detection of metastatic tumors in men with prostate cancer. One imaging agent, fluciclovine F18 (Axumin)—which targets prostate cancer cells in a different way than PSMA-targeted tracers—is already approved in the United States for use in men with previously treated prostate cancer that appears to be progressing (based on rising PSA levels).
PSMA PET-CT is also being studied in this group of men, Dr. Shankar said. One small clinical trial that directly compared PSMA PET-CT with fluciclovine F18 PET-CT showed that the PSMA-targeted scan found more metastatic tumorsExit Disclaimer, regardless of their location. NCI is funding a similar but larger clinical trial.
Dr. Pomper noted that PSMA also is found at relatively high levels in the vasculature of a number of other cancers—including kidney, thyroid, and breast—so he’s hopeful that PSMA PET-CT might be useful beyond prostate cancer.
Researchers at UCLA and the University of California San Francisco (UCSF) have filed separate applications with FDA for approval of a Ga-68 PSMA-radiotracer, according to Jeremie Calais, M.D., of the Jonsson Comprehensive Cancer Center at UCLA. Both applications could be approved by the end of 2020, Dr. Calais said.
However, the respective applications waive any exclusive rights to those tracers, he explained. Once FDA approves those applications, other institutions that have the manufacturing capabilities could produce their own tracers, using the same specifications as the UCLA and UCSF agents, and then undergo an abbreviated approval process with FDA to begin using them, he said.
In the meantime, it’s still unclear how PSMA PET-CT will affect clinical practice in the United States. But it already has in Australia and several European countries, Dr. Hofman said. In Australia, hospitals don’t need regulatory approval to manufacture their own PSMA-based tracers to use in patient care, so at least 60 hospitals in Australia routinely use PSMA PET-CT.
“Urologists and radiation oncologists in many places [in Australia] are already ordering this scan as the standard of care,” he said.
Concerns have also been raised about the costs associated with a broader use of PET-CT. Although costs can vary, in many countries PET-CT is currently more expensive than a CT scan and bone scan. However, if PSMA-targeted PET-CT begins to be more widely used, Dr. Pomper said he’s hopeful that the cost could come down through economies of scale, as has happened for FDG PET-CT, which is the most common form of PET-CT used in cancer.
In the 70s I had a GREAT TIME with Irish doctors coming to the Montreal General Hospital where they had a room next to my standby room. When we were not on duty we used to go and DRINK a lot. One was a dentist named Barney Maloy.
There was another Irish doctor whom I forgot the name that I save his life by giving him 2 shots od adrenaline while he was in anaphylectic shock during a TGIF(Friday party at the residents home) and we were both "ON CALL" so no drinking but a lot of eating & dancing. He ate something that he was severly allergic and started to choke and having my regular set of serynges with different drugs ready for cardiac emergencies and other, so I was ready to help him. It just cut our party short because I told him to come to my ON CALL room which was next to his and asked him to rest on the second bed and I made sure that he was OK.
I learned to live with it since 15 months. So when I was told about my prostate cancer, I just thought it is just another one.
What I was scare was that my PCa vas due to my lymphoma but my doctors told me it was primary, so no connection betwen the 2.
And tomorrow I am telling my haema-oncologist that he will have to transfer my case to the same hospital where I received some fantastic treatments as I did Monday with my ex-chest doctors.
The Cité-de-la-Santé s a newer hosptal, Sorry, my keeoard s screwp.
I got the whole planing of my RT and they irradiated 139.47 cc in the pelvic area and my prostate was only 45.83 cc. And half of my blader received 50 Gy while my prostate and my seminal vesicle got 60 Gy. And the lymphe nodes close to the prostate received also 60Gy. My RO was very agressif versus my agressif cancer.
So I guess they were woried about EPE from my cancer.
The hormonotherapy ADT is getting better now.
How is your husband doing? And you and the children?
Me I would love to know more about my blood relatives so I could have an idea of the medical hereditaries. But I will never know but for my older son, he his not lucky.
Prostate Cancer & Marginal Zone NH Lymphoma from me and Prostate Cancer from his maternal uncle.
My 3 younger sons have just me and their mother (adopted too). Jonathan has Hudgkin Lymphoma, so he could have gotten it from me.
SO I told my 4 sons about the risks of getting these cancers are higher for them and to get PSA testing starting at 45 y.o.
The prostate, the two seminal vesicle, no nerves sparing(irradiated on both sides), all the lymphe nodes in the pelvic area and half the bladder. It may have been less but the ADT that I was supposed to have 8 weeks pre-VMAT was screw-up by the nurse so when I went for the Planning CT where my prostate did not shrink,they had to cover more.
RT are reserved months in advance, I knew the date of my VMAT at the end of March 2020 and with the COVID-19 there was no way to change it and my G(4+3=7) was too agressif.
On the biopsies report there was an invasion perineurale but on abdomino-pelvic CT-Scan and on the bone scan there was no sign of tumor. But I did not have the PSMA scan that looks for microscopic cancer invassion.
Maybe my RO will talk about it. Like he told me: I am a Grade 3.5 but Grade do not use decimal so I am a Grade 3 but I was treated as a Grade 4.
Better that and being over-treated then having a bad surprise.
BTW I found that it is normal that the prostate increase rapidly after the biopsies. It is in reaction to the invasive tests that cause my prostate to go from 24.7 cc to 45.83 cc in 1 month.
Hey doc ! These are all side effects . Feel better .
Hallelujah !! =.03 ... it gets no better than that . Celebrate this great news. Now time to keep that PSA down for many years. I’ve kept mine down for five years now. My prostate was said to be gigantic . I wasn’t a candidate for surgery . I was t-4 which meant my probate exploded with pc tumors ., I came out of that hell . He can do well from here forward. Stay in love !❤️
Please let me know how the shrink goes ? . I went to one . It helped me. At the end of my interview he asked “ what is your reason for living” I pointed to my wife. That was over four years ago now . I pulled out of severe depression as my stats cleared. Still ,I understand. I was groveling on my belly for about three years . You’ve got co morbidities . Although Each one of us is a little different. We are all caught in the same trap . It’s good to seek help . Private chat me up if you like.? We can talk about anything . Love yourself even when you feel like shit . Get through this hard time and things can get better. never give in to bad emotions or APC .🌵
A trip I’d love to take whimpy! Thank you for the invite. You better stick around yourself so you can give my hubby & I the grand tour. Have you been to Ireland yet?
I plan to hold the door open for you .. I’ve yet to visit my grandpas home in Dublin . But my 93 yr old mom did several years back . Heal him up ,get strong ,and don’t predict 5he next step . Relish in the Psa and feed him good food . I am convinced that a holistic diet change helped me greatly .. keep the entire family on a health kick now . Why not ? We want him to ack up many years clear .. it is possible .. stay optimistic and don’t gloom and doom . He’s doing well . Take a deep breath and you’ll both see the Grand Canyon if you wish to ?. Besides our crazy disease the entire world is crazy too. H9ld down down the fort . Better times a head we hope ... 🌵🏜. Scott
Cystoscopy which was supposed to be painless was not. RT caused multiple strictures with some very important.
After the injection of the xylocaine through the penis, he inserted the scope and when he try to go further, I yell due to the pain. So he took it out and got a set of dilators which he used which gradually got more and more painfull.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.