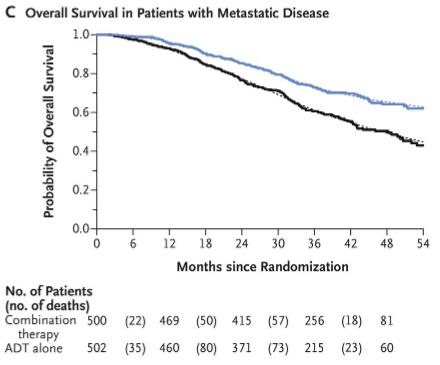
I was doing some research for a possible blog post and came across this survival graph for "early Zytiga" use in metastatic patients from the STAMPEDE trial. If I recall correctly, the 5-year survival for such patients used to be about 28%. This graph stops just short of 5-years, but close enough to make some guesses.
It looks to me like the "don't use early Zytiga" curve is heading towards 40% at 5 years. This would reflect the benefit gained from newer drugs becoming available.
The "early Zytiga" curve is heading towards the high 50s possibly as high as 60%. This would reflect the benefit of using the available drugs sooner and in combination.
This is fantastic! To me it looks like five year survival has now doubled, and there's better than a coin flip chance of living more than 5 years.
Written by
tom67inMA
To view profiles and participate in discussions please or .
One problem that I'm finding is that there is not enough data that indicates what "low volume" compared to "high volume" disease is. Is this a chart that combined both?
I expect so. It's difficult to start sub-dividing because you could do that based on volume, gleason score, PSA at diagnoses, etc., etc. and the combinations would explode.
It's just something I ask myself whenever I see "high volume" vs "low volume". The cutoff many times isn't even gleason, just mets. So sometimes "high volume" is > or equal to 3 mets, sometimes its 5 mets. I've seen a recent study that is putting oligo-metastatic up to 8 mets.
My father started this with around 5 mets. Are one to two small mets really going to push him that much over the edge from low volume to high volume? I know right now he is still sitting at a 0.02 PSA 8 months in. Most of the mets have resolved except for 2 that have persisted since the beginning.
I would just like to see that studies with a greater breakdown and firm definition of what "high volume" vs "low volume" is. So we could possibly see greater precision in care.
I think extent of “Mets” is relative and subjective.
My husband has 4-5 lymph nodes metastatic and at UCLA all drs described him as having “very low disease burden”
And all drs also said that when my father in law was diagnosed with PC in 1990 the prognosis was very poor for 5 year. Survival with distant Mets and that has changed considerably since then. New numbers don’t reflect the extended life expectancies.
I understand that "life is terminal". But it's "how did you die, how did you suffer, and how have you lived".
Knowing that "life is terminal for everyone" really doesn't do anything to ease suffering or to really even motivate me. I remember 7 years ago - i'm 32 now - I had to get open heart surgery to repair a leaky aortic valve. After the surgery, there were 3 wires coming out of my skin because as my sternum was healing, it was pushing the wires out. Combined with the terrible pain of the sternum, my depression because I had to drop out of grad-school at the time and forgo a co-op research effort with Yale, and the fact that i was misdiagnosed for 8 years and it hit my heart strength - I was told by a doctor that "Hey. Let me take you to the cancer ward and show you all the children that are suffering".
I wanted to body slam him through his 300k BMW that was sitting outside. Afterwards, I wanted to say "hey, now let me take you to the cancer ward and show you all the children that are suffering."
I agree with you. And, we can make all of our best efforts at everything, living, avoiding suffering, being our best selves, and this physical life still ends.
My husband is the kindest, calmest, and healthiest stage 4 guy ever. Never a drinker, never a smoker, never a bad thing to say and he has a crummy cancer.
Life is unfair except in death, we are equal in that we all die.
I was told by a doctor that "Hey. Let me take you to the cancer ward and show you all the children that are suffering".
I wanted to body slam him through his 300k BMW that was sitting outside. Afterwards, I wanted to say "hey, now let me take you to the cancer ward and show you all the children that are suffering."}
STAMPEDE conformed with the standard staging definition of metastatic, so they are talking about patients staged as M1 when they say metastatic. They also looked at a small group of men with N1 (pelvic lymph node).
They did have a small sample of recurrent men - it will take many more years to read an overall survival response compared to men who are already metastatic.
My understanding is that locally invaded lymph nodes are not considered to be "metastatic." I had 6 spots in my pelvic area 3 of which have been removed in 3 remain having been identified with a gallium scan. ADT plus radiation treatment is supposed to give me.a.real shot at remission according to UTSW docs. Scholz's group in LA say hit it also with Zytiga/prednisolone. I'm zonked today from radiation every day this week plus a monthly Firmagon shot yesterday. Headed to office to do some work
No Zytiga, I have much of it in hand. Dos here in Dallas convinced me that cancer cells can/will change their DNA to defeat a Firmagon Zytiga/prednisolone cocktail AND the side effects are no free lunch. Completed 4th week of radiation. Some days it (along with Firmagon) kicks my butt
Also, how risky do you think is zytiga, pred combo on someone with stable CAD with 30% plaque in a couple small heart arteries? I have to be so specific but when someone is not specific then people say they can't answer a general question . I read the charter study results which said that people who had very low PSA after 7 months on ADT alone faired best (even better than ADT+chemo) So, I'm guessing that an oncologist might want somebody that's doing well on just ADT to not add anything else..."If it aint broke, don't fix it". I also think my medical oncologist is concerned that adding Zytiga/pred might lower QOL and in turn, cause me to not exercise as much, eat more poorly, be more depressed, which could ultimately result in the same lifespan but with a lower QoL. Your thoughts on that? I realize you are not a practicing doctor. I'm not sure if Heart Artery plaque is a concern with zytiga and pred. That's partly what I'm trying to discern. I didn't notice a major increase in heart events with those adding Zytiga/pred. Did I miss something in the study results? I noticed my MO's name on an xtandi presentation slide at one of the national conferences. Maybe he is biased towards xtandi. I'm not sure why he'd want me to use xtandi first before zytiga, because of my CAD. It seemed like xtandi is harder on the heart than zytiga/pred, based on my readings???
It means that early Zytiga worked equally well regardless of the number of metastases. Sorry, I think your autocorrect made your comments unintelligible. Why is plaque a concern with abiraterone?
I think you misunderstand the CHAARTED study. They only meant that a good response to ADT predicted a good response to docetaxel. I don't know of any relationship between plaque buildup and advanced hormonal therapies. I'm sure you are taking a statin. Exercise is certainly important to maintaining physical and mental health and QOL while on hormonal therapy.
I didn't mean to say that zytiga causes plaque buildup what I was saying is that I have plaque build up already and I'm concerned about the fact that zytiga and prednisone causes higher blood pressure and lot of people in cardiac events as quoted here, which is why I haven't started zytiga and prednisone yet:
" Safety of the abiraterone plus prednisone combination was similar to what has been previously reported, with an excess in grade 4 hypertension with androgen-deprivation therapy alone (20% vs 10%), hypokalemia (10.8% vs 1.2%), and elevated alanine transferase (5.3% vs 1%). Treatment discontinuation due to adverse events was reported in 12% of the abiraterone group and 10% of the control group. Due to an excess in cardiovascular events with abiraterone, Dr. Fizazi urged caution when considering this agent in men with cardiac risk factors."
Hypertension is caused by not taking enough prednisone when one is taking Zytiga. It's just a matter of adjusting the prednisone enough to prevent it. Not a reason to avoid it. This article may help explain the relationship:
I also was wondering how those terms were defined. Also, I was told that
studies only count bone mets, whereas one of my mets was a lymph node. And- some scans are able to detect more mets now than other scans- so comparing the number of mets different patients have may be like comparing apples to oranges, if they didn’t have the exact same type of scans.
Barron they are using the Zytiga with adt for every stage of of the disease. Many cases are not cut and dried metastatic but they use the same plan. Not sure the trial was done the same for everyone but mine was right out of the New England journal of medicine. I found it after it was over.
I was put on Zytiga for 8 months to shrink the tumor before 39 rounds of radiation. I’ll be on it for two years total before going off unless I have a psa rise before my 2 years are up. My tumor was T4 out of the capsule against the rectum. With an mri only it was determined there was no lymph node involvement but a nerve bundle was invaded. The rectum has yet to be determined if it is invaded so it could or could not be. Long story short they don’t know for sure how long we are going to live. I know getting every test possible is the only way to determine the extent of the disease so they can guess a little better. I missed my chance to get a pet scan before they drove my psa down too low to work. Still pissed about that one.
Looks like a combination of newly diagnosed high risk patients and recurrence after treating low risk cancer. All the details are here: nejm.org/doi/full/10.1056/N...
There is another chart from stampede showing a significant benefits in TTDP and OS for low burden metastatic patients who receive RT (like IMRT) to the primary timer along with ADT versus ADT alone. Here’s the article from Lancet:
George, I don’t believe that distinction was made. The conclusion was, ”Therefore, prostate radiotherapy should be a standard treatment option for men with a low metastatic burden.” I’m not sure I understand what you mean by primary tumor being out side the prostate for PCa for low metastatically burdened patients. Can you give an example...
If the prostate was radiated with high dose brachy then the primary tumor is probably dead so anything outside of the prostate, in lymph node/metastatic would then become the primary tumor potentially, depending on how they defined the study.
Median (50%) survival has not been reached with the limited follow-up of the STAMPEDE trial, but we can look at 60% survival and note that the curves are diverging, so the survival improvement is at least this large. In STAMPEDE, early Zytiga increased survival by at least 18 months; In LATITUDE, early Zytiga increased survival by 16.8 months.
Let me make sure I have this straight: the 16.8 and 18 month improvements are versus late Zytiga, which means in addition to the 4 month improvement when used after castrate resistance. Correct?
Does this assume that the adt alone folks are zytiga when the psa started rising in adt alone group? If not, then how do they know whether or not adding it subsequently would work almost as good?
What you say is correct, we are individuals and not a statistic. We won't be 40% dead in 5 years. There's always that guy that refuses treatment, starts eating broccoli, and goes into remission. Yada yada yada.
My takeaway from these studies and statistics are:
1) This is a very serious disease, do everything you can to fight it
2) Using combinations of treatments earlier in the disease process is usually better, but not always. Studies are the best info we have to decide what works and what doesn't.
3) Five year survival has doubled, and that is probably out of date already. Dead men may not post (sometimes their wife does), but in the coming years we should be seeing more and more members living 5, 10, 20, or more years.
Give us $200,000 and we will extend your life by 3 months (maybe)...What a deal ! Where do I sign up for that.?..Oh, and you might not feel to good during those 3 extra months...
Right, and this is exactly what I'm trying to write a blog post about. Elizabeth Warren is saying healthcare is a basic human right but nobody is talking about controlling costs, or having discussions about cost/benefit, etc.
It's great that we're all living longer, but the cost per month is also going up. That $10K a month drug will keep you alive until the $25K a month drug comes on the market. Rinse, lather, repeat. "Medicare for all" by itself won't solve this problem.
Did I mention I'm an independent with a bit of lean to the left?
Hello tom67inMA, Read 𝚈𝚘𝚞𝚛 well-written and thoughtful article. Thank you for sharing. I tried to leave a comment but was unable. My only thought was you may wish to clarify further the concept of “financial toxicity “ ,that it has credibility, and is not only a product of your fine mind.
I have said without anybody contradicting me that the finest health care insurance in the world is worthless if you can't find a doctor. Where are the incentives for people to go into that field?
Consider: you graduate from college. 22 years old. Four years of medical school, internship, residency - you're 29 years old and a quarter of a million in debt and you haven't made a dime yet. I've run these numbers by the CEO of Samaritan Health Services and he confirmed them. He said one of his biggest admin problems is helping the younger doctors in his system with their debt. And all anybody talks about is cutting practitioners' compensation. Already 1/3 of the doctors in California won't take new Medicaid patients; they'd lose money on them.
You've probably noticed that, after initial diagnosis you're more likely to see a physician assistant (PA) or nurse practitioner (NP) than an MD.
Other specialties are worse. There's an infant mortality problem in the US; primarily due to a severe shortage of OB/GYNs. Their malpractice insurance premiums are astronomical so new MDs don't want to go into that field. Midwifery is making a come back.
Nobody is doubting demand for medical services is increasing. It is past time we started thinking about supply. You don't create new practitioners overnight.
You are right on the money. It all starts with the education system. Doctors should get a free education. Whoever scores highest on tests gets to be a doctor. A nice comfortable salary after that. The student debt is the next crisis. I don't think we should have to pay for the $250,000 someone charged up for basket weaving while partying it up and having their rent paid.
Good point. I'm always amazed at the people that do this for me I plan on taking the money that I have and giving it to other people that can use it in their lives instead of wasting it on myself in the last few years.
Did you just tell me to run a lap? LOL! Ya know, I've been Googling all the research into cancer and exercise and... well I better go run two laps now, it's good for me!
As a patient placed on early Zytiga, I am interested in the survival rate of oligometastatic patients that have stereotactic radiation to their met lesions early...will this push OS above 64% and slow recurrence/failure... I am sure an answer is in the works... Thanks for posting...
Overall survival could be influenced by many other pathologies affecting the patients in the study. Many people in those studies died from causes other than prostate cancer. Younger and healthier people with metastatic prostate cancer treated with ADT and Zytiga may have better chances of survival than those indicated by the curves. Those curves do not show a stratification by age or associated pathologies.
When I was diagnosed, I talked to the oncologist about survival statistics, as I'm sure we all did. I asked him if my chances were better because I was younger (55) and in better shape than many men who get prostate cancer. He told me that, while logic would make us think that way, the statistics don't really support that. It really depends on how our individual cancers respond to the different treatments.
When I was diagnosed back in October, during my first meeting with my onc doc I tried to ask him about potential survival time ...... he interrupted me to bring in my wife and introduced us to the Hospice nurse . Dunno f that was an answer to my question or not yayahahaha. Still here tho, and doing better than ever ( ever since I got sick that is ). My onc doc likes to say “ everyone is different “ , guess that’s so.
Since you are younger and healthier than most patients I believe you could probable live longer than the mean OS shown on those curves. Overall survival curves are influenced by age and health status of the people participating in the study. If you do the study of ADT and Abiraterone with people 95 years old or more with multiple associated pathologies the OS would be different when compared with a group of 50 years old patients without associated pathologies treated the same way. Many people in the first group will dye of heart attacks, stroke, pneumonia, old age and some from the cancer. Because of the influence of all these other causes of death the overall survival of that group will be poorer than the overall survival of the second group. Overall survival is not specific death by prostate cancer.
To MarkBC 's point, I suspect that younger, healthier men tend to have more aggressive cancers. This would be due to faster metabolism, more growth hormone, etc. So while they won't be as likely to die of a stroke, they also won't last as long with a marginal response to treatment. Just a thought from a 51 year old with an aggressive cancer.
How are you today after the side effects have subsided? I’m talking about the initial side effects from each treatment. I’m not including the ADT. I know those aren’t any better.
Hey, that's the boat I am in. Stage 4 metastatic, and taking zytiga. Cancer team allowed me to receive radiation to the prostate and bone met as well as this treatment just showed benefit in a trial last year. I figure with the early zytiga, and radiation I might live 7 or 8 years!
I'm also in that boat, but without any radiation to the prostate. I don't have any specific idea how long I will live, but know that it could be for years. That's long enough for things such as diet and exercise to have a significant effect. It's also long enough for new treatments to be approved and new studies to begin.
I can almost guarantee that if you do make it to 7 or 8 years with current treatments, there will be new ones waiting for you to add on even more time.
Yup, a member of my medical team made basically the same point. If we can’t cure it now, the goal then is to keep you around till a cure for it does come.
There are trials going on for stereotactic radiation in oligometastatic disease--initial diagnosis and for recurrence....could possibly buy several years....see page 4:
I have a really good chart prepared by the STAMPEDE team at 3 years which shows the vast difference in OS. Personally, I’m approaching 8 years after a dx PSA of 571. Currently immeasurable.
Unfortunately I can’t find a way to post the image in a response.
Ill be a little more hyperoptimistic than you Tom....at 54 mnths the 'zytiga' graph seems to flatten...dare I say those who make it 54 months can expect a very long survival...lets see what the five year extention looks like...very promising..Thanks for this
My husband has been on zytiga for 8 months and psa continues to drop. What is the average time zytiga works? You aren’t saying zytiga works 54 months? He’s already had chemo .
There appears to be no upper limit for how long it can work. We have members that have been on it for 8 years and it's still working. You won't find stories beyond that yet because the drug is too new.
No..I think you're answering your own question...the zytiga is working if his PSA continues to drop...what I'm hearing is your worried its not working fast enough? We all respond uniquely if so. Whats important is zytiga works well when administered promptly...
The graph is boldly telling us early zytiga treatment outpaces monotherapeutic ADT by 20% at 54 months...50% better results when combined....it gives us no indication of its early results wrt PSA/etc...this is an overall survival graph...the gold standard for treatment evaluation.
I live my life now one day at a time , I love my family and pray daily to thank God for another day. We all have an experation date and only he knows when our milk will spoil.
Trust in your medical team to weigh out your options. I've been in Zytiga, Eligard, Xgeva since day one of diognoses that was 17 months ago PSA 0.1 since first month treatment. I feel pretty good with the usual lifestyle changes that go along with ADT. The trade off is I'm still alive. Never give up never surrender. Leo
I have recently started zytiga based on this research. MO said she has started new patients this year on zytiga based on this research but has to provide this research to the insurance company to get approved.
I had Zytiga as part of a clinical trial. It gave me the longest response I had with medications to this point but lasted about 20 months before PSA started rising. Like it has been stated earlier, everyone is an individual and their cancer will respond as such. The longer you stay around the greater the chance a new Med will show up that will be helpful. Be blessed!
Yes, there's a large number of arms in the study, using letters up to "k" last time I looked. As I recall, the results for Docetaxel were similar to the results for Zytiga, but I couldn't find a graph in a quick web search.
I was Dx with Stage IV PCa in 01/2015, but 10/14/2014 was when I had a PSA @555.2, so using that as my Dx day. 15 Taxotere chemos and 30 months ADT, on Metformin and Lipitor, back on Lupron and PSA went back down to 3.9(840 at Dx)
Hope so. No person is Guaranteed five years of life cancer no cancer I realize his cancer is terminal and it breaks my heart. New medicine is coming out all the time it may not work for him but hopefully you work for someone else don’t know I know my husband is older and five years sounds really good. I realize if you’re in your 50s or 60s five years is not the best but like I said before no one is guaranteed more than the day you wake up I know that I pray every night for every man That’s on this crappy journey
From reading the studies it appeared to be that xtandi resulted in allot more cardiac events than zytiga/pred but my oncologist recommends xtandi before zytiga for me because i have coronary artery disease. What an i missing?
Great chart and like yourself Zytiga is allowing me to live a fairly normal life. I hope that with all the new treatments we can continue to live with advanced prostate cancer and have a good quality of life. 👍
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")