Short but clear discussion on how biomarkers are being used to treat prostate cancer.
1. Biomarkers are used to diagnose PCa and to decide whether or not to biopsy or repeat biopsy.
2. They also discuss how biomarkers are used to treat localized disease and advanced disease.
3. Both tissue and liquid biopsies are used for somatic DNA mutations, with liquid biopsies becoming increasingly important since it gives real-time results.
4. Guidelines for germline testing and counseling are being updated, and germline testing for family members is becoming increasingly important.
5. PARP inhibitors are now approved for detecting BRCA mutations.
6. There is broader approval for the medication olaparib for both germline and somatic testing.
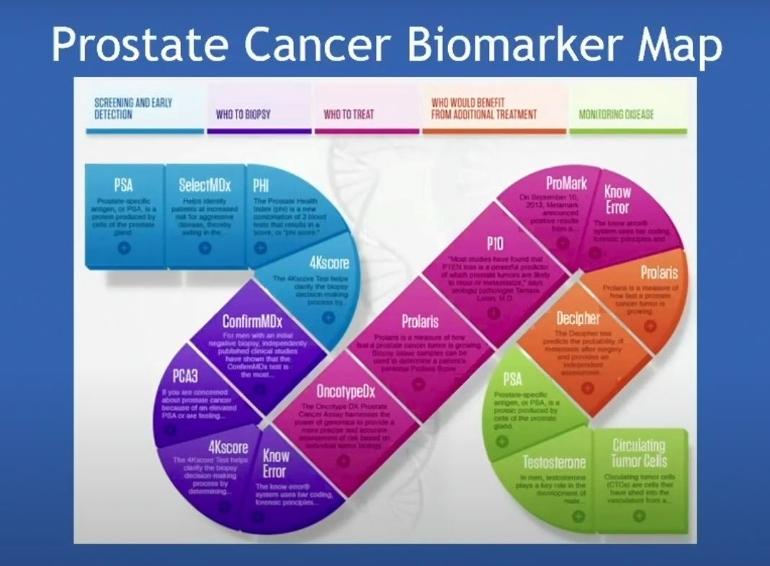
7. They also review the updated biomarker map.
Most importantly at MIN 12:39 they discuss a paper, Welsh PSA, New England Journal of Medicine, that promotes primary care physicians allowing PSA to rise to 10.0 before referring patients to Urologists, or suggesting testing for otherwise non detectable PCa...this was not acceptable to some on the panel of doctors (thankfully) and dominates nearly half the discussion. A acknowledgement follows on how malpractice legal actions for failure to follow up on PSA doubling, not acting on rising PSA, waiting for PSA's to go over 4.0, and being slow to provide screening of affected patients "is the largest source of malpractice lawsuits for all types of cancer in the 18,000 doctors listed in the Harvard Medical School" roster.
Ya think! Waiting for PSA to rise to 10.0 is (in my opinion) madness and should border malpractice. At age 60 your PSA should not be above 1-1.5...otherwise seek testing. In fact I owe whatever advantage I have right now over my PCa to a good friend whose Urologist waited for his PSA to rise to 14 before he bailed, went to a Radiologist and wound up with Stage 4 PCa that was metastatic He then urged me to act at a PSA of 4.1 and get a pMRI...it has made all the difference. Had I not had my friend tell me this my Urologist was happy to do his DRE all the while watching my PSA go up and up and up...if this sounds nuts its because it IS NUTS!
More on point Genomics and Biomarkers may be the way of the future...the MAP created is really cool in that it places all these tests on a timeline, in order of how patients should deploy them. They each have a role and what I dont hear is now patients should deploy 2-3 of them at different points along the treatment path to be able to bracket any PCa that may be lingering...lots to consider.
YouTube LINK: youtu.be/7tA4EGDnG5Q
