Hi all, I had suspected an underactive thyroid so I recently had a medichecks thyroid test. Everything has come back within range with the exception of antibodies which are raised, should I be concerned?
I have an appt with my GP on Tuesday but I'm sort of at a loss because I'm sure they won't care about my symptoms or raised antibodies.
Does anyone have any words of advice?
Written by
Thyroidworries
To view profiles and participate in discussions please or .
So let the GP know you have a positive Thyroid Peroxidase antibody result (TPOab ) .. this is evidence of Autoimmune Thyroid Disease ( immune system is damaging thyroid tissue) , and it means they should keep an eye on your thyroid annually because you are more likely to become overtly hypothyroid at some point in the future .
'Overt' hypothyroid means the TSH is over range AND the fT4 is under range.
'Sub-clinical' hypothyroid means TSH is over range but fT4 is still within range.
NHS can't / won't prescribe Levothyroxine for hypothyroidism until the TSH has gone over range (and stays there at repeat test ~ to rule out a 'one off')
They 'can consider' starting Levothyroxine for 'sub clinical' hypothyroidism IF symptoms are causing a problem (if TPOab are positive it help to persuade them it's going to be necessary at some point anyway , so they are more confident to treat while it's still only subclinical)
Here are the NHS guideline for treating sub clinical hypothyroidism . basically they need two over range TSH results (taken 3 months apart) + symptoms of hypothyroidism , before they can offer you levo.
"1.5 Managing and monitoring subclinical hypothyroidism
Tests for people with confirmed subclinical hypothyroidism (this means 'TSH is over range, fT4 is in range')
Adults
1.5.1Consider measuring TPOAbs for adults with TSH levels above the reference range, but do not repeat TPOAbs testing.
Treating subclinical hypothyroidism
1.5.2When discussing whether or not to start treatment for subclinical hypothyroidism, take into account features that might suggest underlying thyroid disease, such as symptoms of hypothyroidism, previous radioactive iodine treatment or thyroid surgery, or raised levels of thyroid autoantibodies.
Adults
1.5.3Consider levothyroxine for adults with subclinical hypothyroidism who have a TSH of 10 mlU/litre or higher on 2 separate occasions 3 months apart. Follow the recommendations in section 1.4 on follow-up and monitoring of hypothyroidism.
1.5.4Consider a 6-month trial of levothyroxine for adults under 65 with subclinical hypothyroidism who have:
~ a TSH above the reference range but lower than 10 mlU/litre on 2 separate occasions 3 months apart, and
~ symptoms of hypothyroidism.
If symptoms do not improve after starting levothyroxine, re-measure TSH and if the level remains raised, adjust the dose. If symptoms persist when serum TSH is within the reference range, consider stopping levothyroxine and follow the recommendations on monitoring untreated subclinical hypothyroidism and monitoring after stopping treatment."
Tattybogle has explained about your thyroid antibodies and diagnosis.
You might want to give some consideration to your nutrient levels. Hashimoto's (autoimmune thyroid disease) can cause gut/absorption problems which can lead to low nutrient levels.
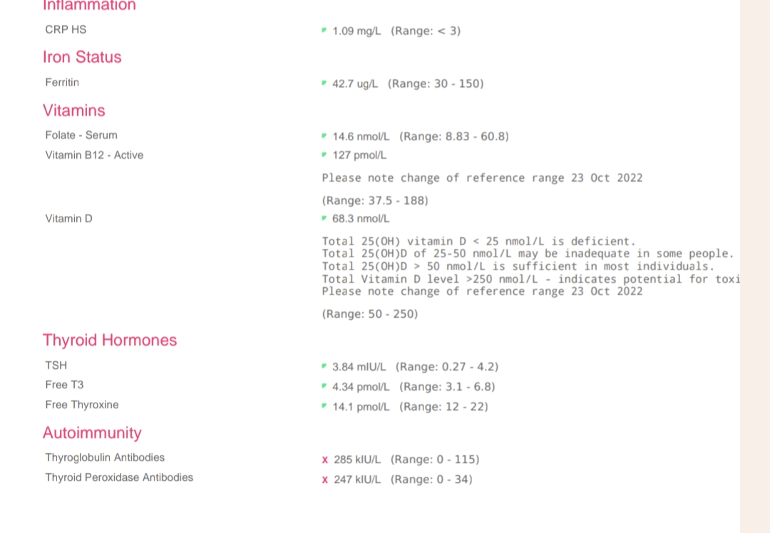
Ferritin: 42.7 (30-150)
This is very low in range. Some experts say the optimal level for thyroid function is 90-110ug/L.
You really need to know if you have iron deficiency or just low ferritin, so you need a full iron panel to include
Serum iron
Total iron binding capacity
Saturation percentage
Ferritin
That test would show if you have iron deficiency.
You can have iron deficiency with or without anaemia, so to see if you have anaemia you also need a full blood count.
You could ask your GP if he's willing to do these tests, but please make sure he doesn't test only ferritin but includes the full iron panel as detailed above.
Folate: 14.6 (8.83-60.8)
This is very low. Folate is recommended to be at least half way through range so you'd be looking at 35 plus with that range. This isn't folate deficiency so your GP wont do anything about it.
You could consider supplementing with a good quality, bioavailable B Complex which contains all the B vitamins plus 400mcg methylfolate. The amount of methylfolate may not be enough so you could add a separate folate supplement temporarily, say one bottle then retest to see how your levels are.
Often recommended here are the following B Complex supplements
Thorne Basic B - can be expensive and often goes out of stock. Good alternatives are
The Vit D Council, the Vit D Society and Grassroots Health all recommend a level of 100-150nmol/L (40-60ng/ml), with a recent blog post on Grassroots Health mentioning a study which recommends over 125nmol/L (50ng/ml).
So now you look at how much is needed to reach 50ng/ml and you'll see that they suggest 3,700iu per day. Nearest to buy is 4,000iu.
Retest after 3 months to see if you need to adjust the dose.
There are important cofactors needed when taking D3.
D3 aids absorption of calcium from food and Vit K2-MK7 directs the calcium to bones and teeth where it is needed and away from arteries and soft tissues where it can be deposited and cause problems such as hardening of the arteries, kidney stones, etc. 90-100mcg K2-MK7 is enough for up to 10,000iu D3.
For D3 I like Doctor's Best D3 softgels, they are an oil based very small softgel which contains just two ingredients - D3 and extra virgin olive oil, a good quality, nice clean supplement which is budget friendly. Some people like BetterYou oral spray but this contains a lot of excipients and works out more expensive.
For Vit K2-MK7 my suggestions are Vitabay, Vegavero or Vitamaze brands which all contain the correct form of K2-MK7 - the "All Trans" form rather than the "Cis" form. The All Trans form is the bioactive form, a bit like methylfolate is the bioactive form of folic acid.
Vitabay and Vegavero are either tablets or capsules.
Vitabay does do an oil based liquid.
Vitamaze is an oil based liquid.
With the oil based liquids the are xx amount of K2-MK7 per drop so you just take the appropriate amount of drops.
They are all imported German brands, you can find them on Amazon although they do go out of stock from time to time. I get what I can when I need to restock. If the tablet or capsule form is only in 200mcg dose at the time I take those on alternate days.
Another "all trans" one worth considering if the others aren't availaable:
Don't take D3 and K2 at the same time unless both are oil based supplements, they both are fat soluble vitamins which require their own fat to be absorbed otherwise they will compete for the fat.
Another important cofactor is Magnesium which helps the body convert D3 into it's usable form.
There are many types of magnesium so we have to check to see which one is most suitable for our own needs:
Don't start all supplements at once. Start with one, give it a week or two and if no adverse reaction then add the next one. Again, wait a week or two and if no adverse reaction add the next one. Continue like this. If you do have any adverse reaction then you will know what caused it.
Some people with Hashi's has found that adopting a gluten free diet helps, but this is not guaranteed.
Supplementing with selenium l-selenomethionine 200mcg daily is said to help reduce the antibodies (but testing first is sensible), as can keeping TSH suppressed.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.