I have felt unwell with hypothyroid like symptoms for about 5 years. Despite this my TSH was always in normal range but had been creeping up over time. More recently my TSH came back as 8.6. My Doctor was still reluctant to help until i'd had another TSH in another 3-6 months that was again high, ideally over 10 to start me on medication.
With me feeling so unwell I started medication from elsewhere and have been taking a quarter tablet of Cynoplus each morning, which is equates to 30mcg of T4 and 7.5mcg of T3 (It's a T4 & T3 medication).
These blood results are from me having been on that medication dosage for 4 weeks. I feel no better. If anything I feel worse, with some days the fatigue being so extreme I can barely get out of bed. I felt some positive effects from the medication in the first 2 days but then nothing.
If anyone has any thoughts on my results and what I need to be doing medication wise it would be greatly appreciate. Bear in mind doctors here are reluctant to help if they see numbers that are in range like these, despite me still feeling very unwell. So any advice you guys have would be appreciated.
Written by
Replenished
To view profiles and participate in discussions please or .
Thanks Greygoose. The things is, I felt some positive effects, day one and two, then nothing This wasn't placebo. I literally had every marker of going from hypo to more normal, then it faded. And weeks on at the same dose, it feels as though i'm now getting worse not better despite bloods going in right direction.When you say undermedicated, do you mean because my TSH is not suppressed or should my Free T3 and T4 be higher?
Wait 6 weeks, book early morning blood test via GP
Alternatively a private consultation with thyroid specialist endocrinologist and get levothyroxine prescribed
Standard starter dose of levothyroxine is 50mcg
Bloods should be retested 6-8 weeks after each dose change or brand change in levothyroxine
Typically dose levothyroxine is increased slowly upwards in 25mcg steps until on approx 1.6mcg per kilo of your weight per day. Unless extremely petite likely to need at least 100mcg levothyroxine per day
ESSENTIAL to test vitamin D, folate, ferritin and B12
What vitamin supplements are you currently taking
When were vitamin levels last tested
Very important to test vitamin D, folate, ferritin and B12 at least once year minimum
20% of autoimmune thyroid patients never have high thyroid antibodies and ultrasound scan of thyroid can get diagnosis
Recommended on here that all thyroid blood tests early morning, ideally before 9am
This gives highest TSH, lowest FT4 and most consistent results. (Patient to patient tip)
Are you in the U.K.?
Private tests are available as NHS currently rarely tests Ft3 or all relevant vitamins
List of private testing options and money off codes
Thanks. I'm not going to come off Cynoplus and wait 6 weeks to get hypo again when I'm already in a bad state. If anything I will go private or tell my GP i've already started thyroid meds and ask if they would prescribe. Clearly Cynoplus has me going in the right direction blood wise though no? Despite no improvement in symptoms other than for the first few days.
The things is, I felt a big improvement for 2 days on the medication. Which i'm assuming was probably the T3 seeing as the effects were so instant. Then unfortunately it faded back to me feeling rubbish again. Why?
Do people do well on Levothyroxine alone? From my reading it appears most people still feel crap on this medication and people often do better with some T3 added?
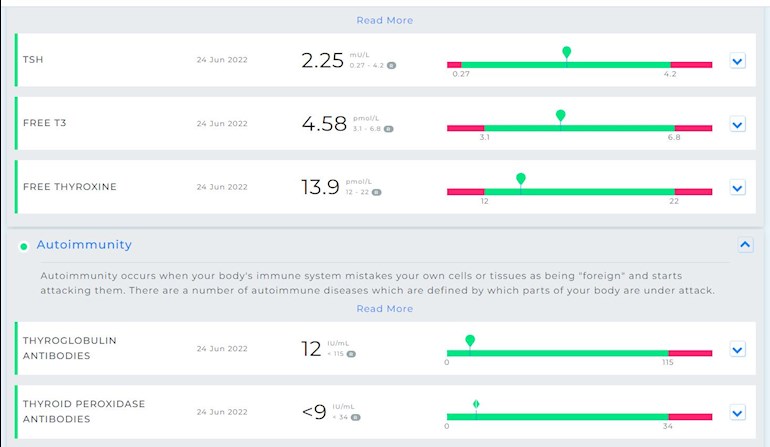
My vitamins were 'normal' / in range. I had these tested at the same time as thyroid as well as many times previously. My bloods were taken in the morning before medication. Results attached.
There’s approx 2 million people in U.K. on levothyroxine
Approx 10-20% don’t do well on levothyroxine…..or more accurately significant numbers of that 20% ….might do ok on levothyroxine for first 5-15-20 years and eventually, often post menopause…..conversion gets worse and then need addition of T3 prescribed alongside levothyroxine
Generally always best to start on just levothyroxine. Increase dose slowly upwards in 25mcg steps until TSH is always below 2, usually around or under 1.
Spoke with my doctor and he's prescribed 25mcg Levothyroxine to start based on my telling him I'd already started thyroid medication in desperation.25mcg...though, that's even less than what I was on and clearly i'm still hypo. He wants me on 25mcg then to test bloods again in 8 weeks. Surely it should be 50mcg at a minimum?
Is there any issue with having some T3 medication in terms of would it suppress my own production and possibly make issues worse? I know you can probably only recommend I follow my doctors advice but I've done that for 5 years and just got sicker.
I'm considering staying on my current cynoplus dose of 30mcg T4 and 7.5mcg T3 in the morning which gives me a little T3 as well as T4 and has clearly started moving things in the right direction, and then taking the prescribed Levothyroxine 25mcg before bed. I'd then be on 55mcg T4 and 7.5mcg T3, which seems reasonable to me.
I think it's obvious from my symptoms and blood results I need more thyroid hormone, not less. I've jeopardised my health for too long waiting for doctors to help.
Yes, the problem with starting T3 too early is almost any dose of T3 will shut your own thyroid output down pretty much completely and TSH will drop extremely low or suppressed
Starting on levothyroxine and increasing slowly upwards in 25mcg steps you have more of a chance of TSH not doing that
In an ideal world, you don’t want a suppressed TSH (and zero thyroid function of your own)
Many people do end up eventually in this situation, once their own thyroid is pretty much kaput….. but if possible it’s better to avoid it.
In the majority of patients 50-100 μg thyroxine can be used as the starting dose. Alterations in dose are achieved by using 25-50 μg increments and adequacy of the new dose can be confirmed by repeat measurement of TSH after 2-3 months.
The majority of patients will be clinically euthyroid with a ‘normal’ TSH and having thyroxine replacement in the range 75-150 μg/day (1.6ug/Kg on average).
The recommended approach is to titrate thyroxine therapy against the TSH concentration whilst assessing clinical well-being. The target is a serum TSH within the reference range.
……The primary target of thyroxine replacement therapy is to make the patient feel well and to achieve a serum TSH that is within the reference range. The corresponding FT4 will be within or slightly above its reference range.
The minimum period to achieve stable concentrations after a change in dose of thyroxine is two months and thyroid function tests should not normally be requested before this period has elapsed.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")