Me a little as I get nowhere after 10 years with hypothyroidism it’s got worse the last two years my GP try’s to blame it on other stuff my thin hair not sleeping anxious panic attacks itchy skin anemic list goes on n on. My bloods did TSH CAME BACK LOW SO BEEN TOLD TO DROP FROM 150 to 100 over medicated normally 150 is ok winter but the fatigued has been so bad the last two years I’m unable to do daily things like a 48 year old should like if I go shopping where I don’t ever sleep n they hate giving zopiclone which I get but I wake up like it’s end of the day I’m just too tired every day now my period didn’t come last week my skin neck face so itchy n scalp any idea if this is symptons of low TSH n is it possible to miss a period of is it now start of menopause. Can we have HRT with Levo can someone explain his low my TSH was I’d appreciate any comments thank you all ❤️
Written by
Freddiestar1234
To view profiles and participate in discussions please or .
some explanations about what the numbers mean and how it works:
TSH (Thyroid Stimulating Hormone) this is just a message from your pituitary gland (in brain) to your Thyroid Gland .. asking it to make more (or less) Thyroid Hormones (T4 and T3).
When everything is working normally ( before we start adding any Levo):
A higher TSH number over 2/3 means "make more please" ,
TSH around 1 means "i'm happy, that's the right amount"
TSH of 0 means "stop making any more for now, we've got a bit too much"
T4 is the inactive/ storage / transport form of thyroid hormone. the level of this is tested in a test called fT4 (free T4) which measures how much T4 is freely available to be to used.
When our thyroid is damaged or missing, and can't make enough T4 for us anymore, we are prescribed levothyroxine . which is a synthetic copy of T4.
So once we take Levothyroxine the fT4 test measures the T4 made by our thyroid, plus any T4 we added with Levo.
Your fT4 result means :
17.7 [12-22] ~ 95% of healthy people will have fT4 level somewhere between [12-22] on this [range].
You have 17.7 , which is in the middle , not higher or lower than most healthy people. But where people feel best on this 'range' is very individual .
eg Somebody might need 21 to feel well , and if they had only 13 they would feel very hypothyroid.
Somebody else might only need 15 to feel well , and if they had 21 they would feel hyperthyroid.
The GP will say "you are in the 'normal fT4 range' so that's OK" , but you wont feel OK unless you have the right amount for you.
It's like shoe sizes... size 6 shoes are only comfortable if you're a size 6, but not much use of you're a size 7and a half..... but a GP might say . "but size 6 shoes are very 'normal' for adults so they'll do"
T3 is the 'active' form of thyroid hormone that works inside your cells, in nearly all parts of your body, to make your body function
T4 is converted into T3 , inside your cells . And the thyroid gland also produces a bit of T3 for instant use.
'Too much T3' is what causes Hyperthyroid (overactive) symptoms ,and Too little T3 is what causes Hypothyroid (underactive) symptoms.
Your fT3 hasn't been tested, because the NHS hardly ever test it unless they think you've got too much of it and are Hyperthyroid, ....But it' the most important test really , because T3 is the only one that actually 'does' anything, if you don't make enough T3 for your needs you don't work properly.
Your Doctor is saying you are taking too much T4 (from Levo ) because your TSH is very low.
In a healthy person a TSH of 0.03 WOULD mean they were making too much thyroid hormone. Just looking at TSH on it's own is usually good enough to tell whether there is too little or too much thyroid hormone... but this is only true in healthy people.
But once our thyroid is damaged , or we had graves, and we are taking replacement thyroid hormone, there are other reasons for TSH to be that low, and it doesn't always mean you are taking too much Levo,
The regulating system doesn't work quite the same once its been messed about with by having Graves or by taking thyroid hormones . So then you have to look at not just the TSH message , but also look at what the actual thyroid hormone levels are (fT4 and fT3) AND what symptoms you have, to tell you if you need to take more or less thyroid hormone.
Your TSH say's "you're taking a bit too much", BUT your fT4 says "you're only half way up the range, so not taking too much at all, might even need to take a bit more"
So on here, lots more details will be asked for, to help find out whether you really are taking more T4 than you need, or whether your TSH message has got it a bit wrong.
Sorry that turned into an essay ... I hope some of it is helpful. Xx
(p.s when answering questions here , make sure people realise you've had Graves and RAI as it affects the answers )
What a kind helpful message thank you so much. I ask for T3n T4 ti be tested n she moans but how often if I pay for tests should I test myself so I don’t know what my T4 T3 is my last tests my haemoglobin was low she didn’t tell me n my iron was low again everything else I think was ok so I need educating on privates tests n how much n how often n is it worth looking into T3 but who do I get it off I dare ask my gp she huff puff blow the surgery down lol
Your haemoglobin is well in range, showing that you are not anaemic.
Your MCV is bumping along at the bottom of the range. This is telling you that your red blood cells are small. MCH is likely to be low if MCV is low - they mirror each other.
Small red blood cells are found in cases of iron deficiency. I would suggest that you get an iron panel done. People can have iron deficiency OR iron deficiency anaemia. Iron deficiency needs to be treated with or without anaemia if you are to have a hope of feeling well. But unfortunately doctors often don't notice low or high levels of blood tests if they are in range, so I doubt your doctor even noticed that your MCV was very close to the bottom of the range.
You could bring the low MCV to your doctor's attention, but since your level is in range there is a very good chance that you will be told it is "normal". You could ask for an iron panel to be done. If the doctor won't do this then it is possible to buy an iron panel test :
One of the biggest problems that people have with low levels of iron is that, if it is tested and shown to be low then doctors might prescribe iron supplements. Then, perhaps two or three months later they may test ferritin (iron stores). If it has risen then the doctor thinks "job done" and stops prescribing iron pills. The patient's iron and/or ferritin levels drop and they end up with low iron again. Then doctor might re-prescribe but I wouldn't bet on it. And so it becomes a vicious circle with the patient spending a lot of time with low levels of iron.
In the UK people can buy iron supplements without prescription from pharmacies. Iron is poisonous in overdose so great care must be taken in supplementing. And once someone has reached mid-range for either ferritin or serum iron then reducing dose of iron supplements to a maintenance level is essential.
So the first thing that is obvious to say .... the suggested reduction from 150 to 100mcg ...... that seems like far too big a drop in dose. If a reduction is needed at all , your dose of Levo should only be reduced by 25mcg at a time, (at the most)
i think reducing to 100mcg will be big shock and probably leave you feeling very under medicated after a week or so.
It would be much better to reduce to 125mcg (or 137.5mcg) and then retest after a couple of months on that dose .
Ask the GP why they think you need such a drastic reduction .
You fT4 is not over range, ( it's right in the middle of the range about 50%).....so even of you are a bit overmedicated on 150mcg , it's not by much.
if you feel lousy it's always worth trying a slight dose reduction for a few months to see if it improves how you feel .
I'm too tired to think clearly now , but i'm sure others will be able to put together a much more helpful reply for in the morning.
There are reasons why a low TSH doesn't always mean you are overmedicated, and other things to check ,, but i can't get my brain of fingers to work well enough to explain them just now
So night night for now ..and welcome to the forum.
ALWAYS test thyroid early morning, ideally before 9am and last dose levothyroxine 24 hours before test
Is this how you did this test
Request GP test vitamin D, folate, ferritin and B12 levels BEFORE considering reducing dose levothyroxine
For full Thyroid evaluation you need TSH, FT4 and FT3 plus both TPO and TG thyroid antibodies tested.
Important to test vitamin D, folate, ferritin and B12 levels at least once a year
Are you currently taking any vitamin supplements?
Do you know if you have high thyroid antibodies
Low vitamin levels are extremely common, especially with autoimmune thyroid disease (Hashimoto’s or Ord’s thyroiditis) usually diagnosed by high thyroid antibodies
Autoimmune thyroid disease with goitre is Hashimoto’s
Autoimmune thyroid disease without goitre is Ord’s thyroiditis. Both are autoimmune and generally called Hashimoto’s.
In U.K. medics never call it Hashimoto’s, just autoimmune thyroid disease (and they usually ignore the autoimmune aspect)
Recommended on here that all thyroid blood tests early morning, ideally before 9am last dose levothyroxine 24 hours before test
This gives highest TSH, lowest FT4 and most consistent results. (Patient to patient tip)
Private tests are available as NHS currently rarely tests Ft3 or all relevant vitamins
List of private testing options and money off codes
Freddiestar1234 The places for private testing are in SlowDragon reply (above this one)
ask slowdragon which is the best one for you to use.
(the cheapest is Monitor My Health if you just need TSH ,fT4 and fT3 ,it's less than £30, but if you also need to test Vit B12 / Vit D /Folate /Ferritin then one of the others will be better)
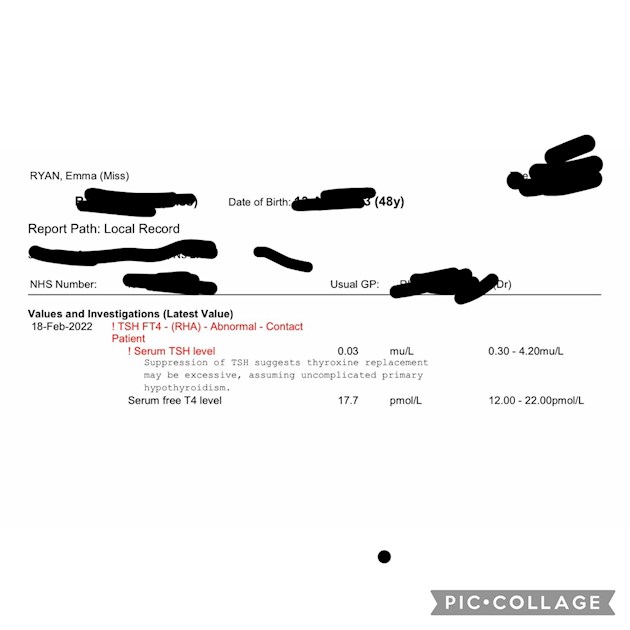
I have copied the 'out of range' results from your pictures below so people who know more than me can read them easier :
Anaemia for 28 ys
48 yrs old Graves / RAI /Levo ...10 yrs ago.
Unwell last 2 yrs. Insomnia.. COVID Dec '21...Itchy skin last 2 weeks ..missed period.
150mcg Levo ..... been asked to reduce to 100mcg due to :
latest test : (on 150mcg)
TSH 0.03
fT4 17.7[12-22]
Previous test :June '21 (on100mcg)
TSH 3.5
fT4 15.5 [12-22]
Ferritin 26[13-150]
other * results from June '21
*Hb 109 [115-165]..... 58 in May '21
*MCV 74.4 [78-98] ..... 68.3 in May
*MCH 22.1 [27-32].... 22.5 in May
*MCHC 297 [310 - 360]
*red blood cell distribut width 17.7 [11.5-16]
Freddiestar1234 .... don't worry about understanding Antibodies for now , they are not so important for you .... they are to find out what caused the hypothyroidism , but we already know Graves followed by RAI is the cause of yours.
Please don't reduce your meds without a LOT more testing. Once you are on levo, it doesn't matter at all if TSH goes under range (although most GPs don't kno enough about thyroid so think it is all-important). What matters MUCH more is your actual thyroid hormones - and your free T4 is only 57% through range. Most of us need it MUCH higher than this ... a good 75% or more, and for free T3 (not tested) to be at least 2/3 through range to feel good.
It also sounds as if your key nutrients aren't great - so as the GP to test ferritin, folate, vit D and B12 (I'v had some success with mine by saying that these tests are recommended by Thyroid UK).
Remember, always an early morning (before 9am) fasting blood test (when TSH is highest), 24 hours from your last levo (so you have a good representative level of hormone in your blood rather than a just-taken-your-meds spike)
And tattybogle is right - even if you DID reduce your meds, such a huge reduction will only make you really ill - and may not impact your TSH anyway. When I was on levo -only, I was fine on 150 x 4 and 125 x 3 but felt awful on 150 x 2 and 125 x 5 although it's only a tiny decrease (and didn't change my blood results at all either) x
I don’t think I’ve ever been tested antibodies what is that. I’ve sent over few full blood tests from may n july n the. Obv the one yesterday was just for TSH so not sure what allThe other tests r as I don’t understand lots of it sadly I try google n learn etc but I’m never sure but I know I feel very heavy arms can’t sleep n just overly fatigued
The biggest single cause (90%+) of hypothyroidism (under-active thyroid) is Hashimoto's or Hashi's. This is indicated by high thyroid antibodies, which it's why it's worth testing them. Hashi's is therefore really common - but it can't be cured (so it's not worth re-testing if you have had high antibodies once). And your antibodies will go up and down as they please - if you DO re-test and find them lower than before, it doesn't mean you're "getting better" - they'll just bounce up later. BUT a lot of people with Hashi's find it helpful to go (strictly) gluten-free - even if not coeliac - and/or lactose-free. And some people have a "Hashi's flare" which makes them "feel" very hyper - and their blood results temporarily go "crazy-high" as if they ARE hyper. [If that happens, you shouldn't change your "base" meds, just atop altogether for a few days til the flare if over].
greygoose does a great summary of Hashi's so am flagging her here
And yes, there's a raft of thyroid terminology to get to grips with. It's worth a read of the hypo section of the main Thyroid UK site - and helvella does a great glossary - now, I think included in his "vade mecum" in pinned posts - which is a better bet than a random trawl through the internet, as you can rely on it to be accurate
Do you always get your blood tested at the very earliest a.m.? It is a fasting test (you can drink water) and don't take thyroid hormones before blood draw but take it afterwards with one glass of water.
Request GP to test B12, Vit D, iron, ferritin and folate too.
In all people, a serum ferritin level of less than 30 micrograms/L confirms the diagnosis of iron deficiency
Look at increasing iron rich foods in diet
Eating iron rich foods like liver or liver pate once a week plus other red meat, pumpkin seeds and dark chocolate, plus daily orange juice or other vitamin C rich drink can help improve iron absorption
This is interesting because I have noticed that many patients with Hashimoto’s disease and hypothyroidism, start to feel worse when their ferritin drops below 80 and usually there is hair loss when it drops below 50.
Thyroid disease is as much about optimising vitamins as thyroid hormones
Never supplement iron without doing full iron panel test for anaemia first and retest 3-4 times a year if self supplementing. It’s possible to have low ferritin but high iron
None of those tests have any direct bearing on thyroid. However, from my limited knowledge of iron - which is very complicated! - it rather looks like you many have low iron, but I can't swear to it. We need someone like humanbean to interpret all that.
Certainly there are no antibody tests in all that. But, just for your information, this is a brief run-down of Hashi's:
OK, so Hashi's is an autoimmune disease – commonly called by doctors Autoimmune Thyroiditis - where the immune system attacks and slowly destroys the thyroid. It is diagnosed by blood testing Thyroid Peroxidase (TPO) antibodies and Thyroglobulin (Tg) antibodies.
(It's necessary to understand that the blood test to see if your hypothyroidism is autoimmune might not give you any further information, for three reasons:
* What they are testing for are TPO antibodies. Antibodies fluctuate all the time, so one test might be negative, and the next positive. But, if you have one over-range test, it does mean you have Autoimmune Thyroiditis.
* There are two types of Hashi's antibodies: TPOab and TgAB. The NHS only tests TPOab, and they might be negative, but if your TgAB are positive, it means you have Hashi's anyway.
* Some Hashi's people never even have over-range antibodies. They are diagnosed by ultrasound. So, a negative antibodies blood test does not mean you don't really have it.)
There are two types of Autoimmune Thyroiditis: Ord's and Hashimoto's. But, we call them all Hashi's for convenience. The difference is, that with Hashi's, you have a goitre, with Ord's you don't. But, the end result is the same: a dead thyroid.
Contrary to popular belief, it is not the TPO/Tg antibodies themselves that attack the thyroid:
"When lymphocytes infiltrate the thyroid gland, mistakenly taking it for a foreign bacteria invader, they damage the thyroid gland and release thyroid peroxidase &/or thyroglobulin into the blood stream. These don't belong outside of the thyroid gland so antibodies are developed to mop them up.
The antibodies are a result of the attack on the thyroid gland, the antibodies don't cause the attack."
After every immune system attack on the thyroid, the dying cells release their stock of thyroid hormone into the blood stream, causing the levels of the Frees to shoot up - FT4 to around 30 something, FT3 around 11/12 - and the TSH therefore drops to suppressed.
There is no knowing how long these high levels will persist, but eventually, they will drop by themselves as the excess hormone is used up or excreted, and not only will you become hypo again, but slightly more hypo than before, because there is now less thyroid to make hormone.
(NB: A Hashi's 'hyper' swing is not true hyperthyroidism in that your thyroid is over-producing thyroid hormone. It's physically impossible to 'go hyper' if you are basically hypo. The thyroid cannot regenerate itself to the point of over production of hormones - or even normal production. Very few doctors appear to know that.)
Therefore, it's very important that your doctor does not reduce your prescription, because you’re going to need it again! If you start to feel over-medicated at that point - some do, some don't - the best thing is to stop levo for a few days, then, when you feel hypo again, start taking it again. It's very important to know one's body, and how it reacts.
There is no cure for Hashi's - which is probably one of the reasons that doctors ignore it - apart from the fact that they know nothing about it, of course!
However, between the 'hyper' swing, and the descent back into hypothyroidism, there can be a phase - quite a long one, sometimes - of normality, where the person is neither hypo nor 'hyper'. This is where people sometimes start talking of having 'cured' their Hashi's, by whatever means. But, it doesn't last. Eventually, you will go hypo again.
But, there are things the patient can try for him/herself to help them feel a bit better:
a) adopt a 100% gluten-free diet. Hashi's people are often sensitive to gluten, even if they don't have Coeliac disease, so stopping it can make them feel much better. Worth a try. Some say that going gluten-free will reduce antibodies – I’ve never seen conclusive proof of that, but, you should be aware that even if you were to get rid of the antibodies completely, you would still have Hashi's, because the antibodies are not the disease. It is not the TPO/Tg antibodies that do the attacking.
b) take selenium. This is not only reputed to reduce antibodies, but can also help with conversion of T4 to T3 - something that Hashi's people often find difficult.
c) the best way to even out the swings from hypo to 'hyper' (often called Hashi's Flares, but that doesn't really sum up the way it works) is to keep the TSH suppressed. This is difficult because doctors are terrified of a suppressed TSH, for various false reasons, and because they don't understand the workings of Hashi's. But, TSH - Thyroid Stimulating Hormone (a pituitary hormone) - tries to stimulate the thyroid to make more hormone, which also stimulates the immune system to attack. So, the theory is, the less gland activity there is, the less immune system activity there will be, meaning less attacks, gland destruction slowed down and less swinging from hypo to hyper and back.
As to your main problem with your GP, he is very, very ignorant about thyroid. He is going to make you worse and keep you sick because he doesn't understand how any of it works. Is there someone else you can see before too much damage is done?
U know I’ve never ever been told any of this it’s only due to great places like this or google I never fast n my blood tests r always In afternoon as I can’t get out of bed I’m so fatigued it’s quite embarrassing when I make appts with anyone urs gotta be after 1-2pm u don’t know what optimal range means or anything was u def royal free once for not then got discharged as I was c quite well had a very active job for 10 years it’s the last two years that’s killed me im just not the same person anymore n if I ask my gp she says it’s not ur thyroid I’m anemic been anemic 28 years been in hosp dm several times very ill without sleep I feel no one can reoair n feel good I don’t want to keep taking sleeping tablets n that’s a huge prob asking she hated giving them so I’ve not been taking themThe last few weeks my skin is so itchy my scalp my neck face I just think what a crap life I lead sometimes I see my mates family doing normal stuff. But my gp seems to huff puff if i mention how I feel there ringing me on Monday n I’m gonna insist to get referred back hosp. I like to know more about T3 as Levo don’t help me all my doctor wants to give me is anti depressants n they affect me very very bad tried 6 different types n I can’t get passed day 2/3 Feel kinda thick I don’t seem to understand how hypothyroidism works I know hair loss nails no sleep etc but managing it nothing works I’m too tired to take at 7am when my alarm
Goes off so stated taking it night but then I think I snack n I’m messing the absorption up so I’m back to taking it 7-8am. Sorry fir the long message n thank you guys always so helpful on here ❤️
When you got these results did your doctor tell you that you were anaemic? Since it would appear from the later results that you were put on iron then I'm assuming you must have been told.
Your Haemoglobin (Hb) is well under range, and your Mean Cell Volume (MCV) is also well under range. The Hct (Haematocrit) and MCH (Mean Cell Haemoglobin) are below range because they are either calculated from your Hb / MCV or they mirror the Hb / MCV.
Hb is what gives your red blood cells their red colour. The reference to Hypochromia on the first sheet is indicating that your red blood cells are paler than usual. The MCV is a measure of the average size of your red blood cells and yours are small and this is indicated by the reference to Microcytosis.
Both Hb and MCV should rise with iron supplements.
June 2021 results
Your Hb and MCV are still low but have improved since the previous month. I see that you were put on iron and it has improved some of your numbers. I'm not sure I understand RDW, but I think the raised RDW shows that your body has started producing some new red blood cells, and they are very different in size to the ones you had before (which were too small). I'm assuming that this is because of the iron.
July 2021 results
Your ferritin (iron stores) result of 26 was still far too low for good health. But refilling your iron stores when you've been extremely low in iron can take months or even longer. (It took me nearly two years to raise my ferritin to mid-range when mine became very depleted, but people do absorb iron at different rates.) Ideally your ferritin would be mid-range or a little bit over. So, with the reference range you've been given you would ideally have a result somewhere between 80 - 110.
Are you still taking iron supplements? If yes, what are they and at what dose?
Your TSH at 3.5 is far too high for someone who is taking thyroid hormones. For most hypothyroid people it needs to be around 1 or less. To lower your TSH you would need a higher dose of Levo.
Your Free T4 is only 35% of the way through the range and most hypos need it to be in the upper half of the range. So at the time these results were done (July 2021) you were under-medicated. Did you get an increase in your dose? I see that you mention in your post that your doctor is planning to reduce your Levo from 150mcg per day down to 100mcg per day. What was the sequence of events? Did your doctor raise your dose in July 2021 and it has reduced your TSH so now he/she is panicking and saying you are over-medicated?
I think a reduction from 150mcg to 100mcg is a shocking over-reaction. Your Free T4 is only 57% of the way through the range. That might be okay for some healthy people, but for many hypothyroid people it wouldn't be enough. Once you are on thyroid hormones for hypothyroidism the TSH is really not a useful test, even though doctors (sadly) think it tells them everything they need to know.
You wrote :
I get nowhere after 10 years with hypothyroidism it’s got worse the last two years my GP try’s to blame it on other stuff my thin hair not sleeping anxious panic attacks itchy skin anemic list goes on n on.
The symptoms you mention - the thin hair, not sleeping, anxiety, panic attacks are very similar to the symptoms I had when I was very low in iron. Under-medication for hypothyroidism will make all those symptoms worse too. The itching could be caused by intolerance of the brand of Levo you are taking. A change of make would be a very worthwhile experiment.
...
Regarding iron supplements, they can be bought without prescription from pharmacies in the UK. I've listed the available options in this reply to another member :
My personal experience of iron deficiency/anaemia is that doctors will stop prescribing long before the patient has reached adequate levels of iron, and got haemoglobin etc. I ended up teaching myself what I could about iron and anaemia and then buying my own iron supplements without prescription. Once I'd got my ferritin to mid-range, my serum iron was still low. I chose not to push my ferritin higher, and reduced my iron pills to a maintenance dose. I stayed on a maintenance dose for several years, adjusting up and down as necessary to keep my ferritin around mid-range, until another health problem intervened and I had to stop taking it.
Anyone taking iron needs to test fairly regularly to make sure they aren't overdosing. Iron is poisonous in overdose. A few links that you might find useful :
Thank you so much for allThat info it’s been really helpful I don’t think since covid I’ve been seen enough regarding blood tests I feel like I’m bugging my GP so I’m
On iron tablets which I’ve been on n off for last the 20 odd years but when I’m ok them I’m not told to go back so I just stop them
After the time I was given n then blood tests r only re done if I ask so since July one I don’t think tested for it I take 200 mg of them n so I must ask tomorrow for a full vitamin tests iron is there any thing else I should ask for
Sorry toAsk again my t4 57% is that not good what should it be as my GP only flagged up the low TSH she never gives me anything lower than 25 mg so it’s hard to break those small tablets at times
I’ve also been prescribed amitriline to help sleep. There old fashioned anti depressants which has helped with moods depression slightly but not sleep I was wondering if it’s them that’s clashing with Levo does anyone know I looked them up n it says yes n other google searches says no my fatigued is just all the time I’m finding I’mHome more n more now
I was never told myHaemoglobin was low I saw it n looked it up she never commented on that I was taken into hosp in the may reason I had all those tests done after covid 2nd jab I had a period n bleeding wouldn’t stop the hosp couldn’t stop it even after drips of transit acid after few days it eventually stopped n I’ve never really picked up from that admission
Summer I’m left to be on 100 mg n winter 150 n if I say I’m feeling cold tired she will say well your last test was fine nothing wrong I’ve adjusted it here n there Since july n I felt better for week or twoThen I’m fatigued again so I get confused if I’m tired I assume meds needs lowering or increasing ? There called by accord ferrous Sulfate
Yes . i think you should stay at 125mcg for 6 weeks and then get a new test . Don't agree to reduce any further until you see what your results on 125mcg are.
freddiestar1234 . Just Checking .....i assume you have been told by the Doctor to make sure you take any Iron supplement well away from your Levothyroxine ? (at least 4 hrs i think ?)
otherwise the Iron means you don't absorb as much T4 from Levo tablet ....( meaning your T4 would go down and your TSH would go up)
If vitamins are very low …..working on improving them, retest in 3-4 months see if need further improvement
Once you get vitamin levels improved by supplementing, maintain at optimal and steady levels, can then usually just retest vitamin levels once a year
Common to need ongoing supplements as maintenance dose
Retest thyroid levels 6-8 weeks after any dose change or brand change in levothyroxine using cheaper Monitor My Health test - just TSH, Ft4 and Ft3 at £26.10 if need to test in between annual full test
Hi all just amUpdate I’m sticking to 125 from 150 instead of the 100 my gp advised me to
They called me up yesterday after I had a moan n they made me go today at 12 for a full blood count whether it’s involved T3 T4 I’m not sure but my period came yesterday n today I’m feeling terrible. I shall let u all know my results when they arrive then I can order the kits privately Thank you all once again ❤️
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")
")