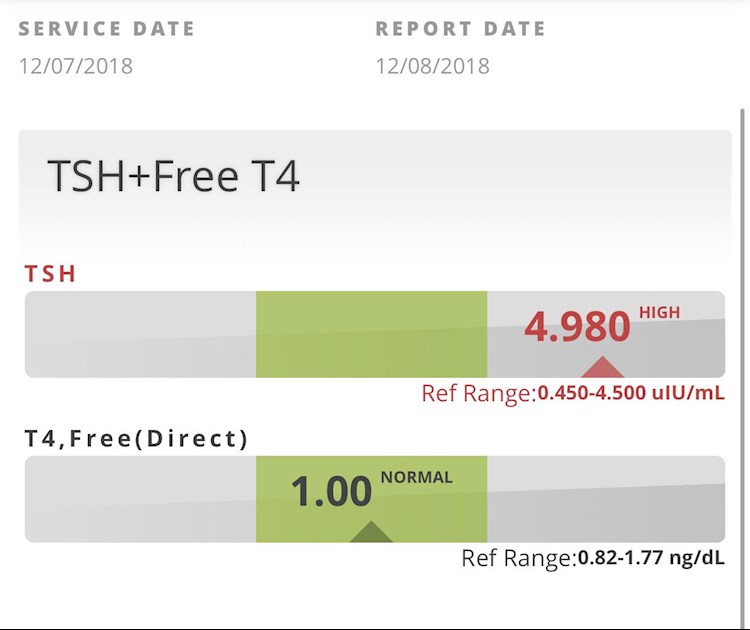
Well husband since thyroidectomy in August and had parathyroid removed also he has gained 49 lbs here are his current labs he takes Levothyroxine 112mcg and they are adding another half tab on Sunday’s only ?
Help with labs: Well husband since thyroidectomy... - Thyroid UK
Help with labs
Written by

Tru4hockey
To view profiles and participate in discussions please or .
Read more about...
1 Reply
•
SlowDragonAdministrator
After thyroidectomy TSH should be around one and FT4 towards top of range and essential to test FT3
For full Thyroid evaluation you need TSH, FT4 and FT3 plus both TPO and TG thyroid antibodies tested. Also extremely important to test vitamin D, folate, ferritin and B12
Low vitamin levels are extremely common and often need supplementing
All thyroid blood tests should ideally be done as early as possible in morning and fasting. Do not take Levothyroxine dose in the 24 hours prior to test, delay and take immediately after blood draw. This gives highest TSH, lowest FT4 and most consistent results. (Patient to patient tip, best not mentioned to GP or phlebotomist)
He's likely to need 125mcg daily. Retesting in 6-8 weeks.
If TSH is still higher than 1.5, then a further increase
Suspect you are not in the UK?
Dr Toft, past president of the British Thyroid Association and leading endocrinologist, states in Pulse Magazine,
"The appropriate dose of levothyroxine is that which restores euthyroidism and serum TSH to the lower part of the reference range - 0.2-0.5mU/l.
In this case, free thyroxine is likely to be in the upper part of its reference range or even slightly elevated – 18-22pmol/l.
Most patients will feel well in that circumstance. But some need a higher dose of levothyroxine to suppress serum TSH and then the serum-free T4 concentration will be elevated at around 24-28pmol/l.
This 'exogenous subclinical hyperthyroidism' is not dangerous as long as serum T3 is unequivocally normal – that is, serum total around T3 1.7nmol/l (reference range 1.0-2.2nmol/l)."
Professor Toft recent article saying, addition of small dose of T3 may be necessary for many. Note especially his comments on current inadequate treatment following thyroidectomy
Not what you're looking for?
You may also like...
Help interpreting lab results please!
Levo only medication. Endo has me on 75mg Levo and 10mg T3. After reviewing me at his clinic, here...
urgent help required with thyroid labs
psoriasis
depression
joint pain
low libido
weight gain around the abdomen
Bloating after...
Needing help with lab results please
latest labs while taking 88 mcg T4 for 2 months, taken while fasting, and no T4 the day of labs. I...
Desperate for help interpreting my labs.
etc ) I decided to take matters into my own hands and pay for a test which also tested for thyroid...
Please help with lab results! I need answers!
stairs now. I'm not that old am I?! I've gotten labs done and just got the results from my MD. I...