(not paste my question into CHATGPT which I could do myself in 10 seconds if I wanted a banal homogenized reply not from a knowledgeable subject matter expert)
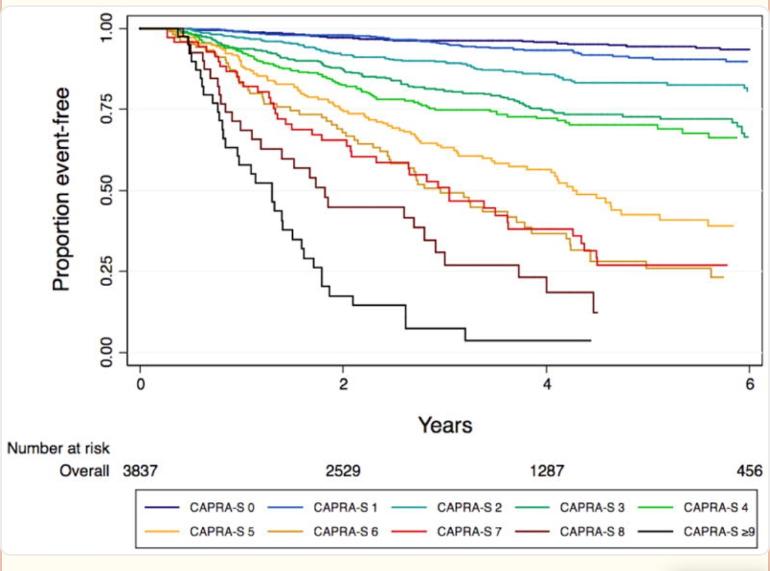
why for high risk post RP cases non metastatic there seems like a big difference in predicted outcomes. This graph is CAPRA-S score vs a group of RP patients and for high risk (black line) almost nobody makes it without recurrence within 4 years but with example high risk parameters (g9 svi, epe, high psa pre op) when I use MSKCC recurrance calculator It comes up with a much less dire prediction if one is undetectable post op, IIRC about 50:50 odds of 5 years no recurrence. Negative margins etc can still be high CAPRA-S score. Obviously I would like to believe the MSKCC nomogram but this study of CAPRA-S scores says otherwise.
I have no special expertise I just read the paper so these are guesses.
One obvious difference is that the mskcc uses post op psa which is probably a strong predictor.
Capra s is older and based on older data. Perhaps post op psa wasn't as reliable then?
Lni given 1 point seems low and my guess is that is very low volume, otherwise they would have received adjuvant RT and been excluded.
Maybe PLND and ePLND is more used today?
SM isn't really just binary, positive SM GS8 is different from GS6.
It seems a small sample especially considering the number of variables.
Practices and staging have evolved since 1992. Better imaging would have possibly moved less favorable patients towards RT. This effect is probably more pronounced with RT improvements.
I didn't look at how mskcc arrived at their model but I suspect it would be more reliable.
thanks, I hope you are right. Since the graph “to recurrence event” starts at near 100% presumably those with post op psa failure were not on that line - as their “event” was immediate, so to speak.
Even with 0 months undetectable under the belt, as input, MSKCC Is still more optimistic. For my high risk category, anyway.
What is your "risk category"? Perhaps someone on here has been down that road, so to speak, and can give you some actual results? For my pathology, both of these models pretty much line up with each other. IIRC, margins are not considered very much in prediction models unless they are positive. A negative SM patient can still have EPE, LVI, SVI, LNI etc.
g9 4+5 epe svi 35ng 0.01 neg margins after rp. that puts me on the black line in the graph above which if I was in that study, would give me 10% chance of being recurrence free by 4 years.
What % of PV was involved? Also, how many months are you .01 after RP? That appears to be the big indicator....time at a lower USPSA after RP. Also that black line represents ONLY those patients that fell under CAPRA definition of BCR which was .2 or above within 6 months following surgery. So IF, you are further along than 6 months and still at .01 you wouldn't necessarily be represented accurately by the black line?
maybe I am misunderstanding the black line. It starts at RP with the bad capra score confirmed by operation and pre op psa. then as people go BCR ( > 0.2) it drops. So if I was in the study, I would be in a cohort where 90% plus fail with BCR after a few years. As I am now at 2 years, I would be already in the still rapidly shrinking class of just 20% remaining still <0.2
whereas the MSKCC calculator would have told me after RP I was like 60:40 for recurrence in, I think they quote for 5 years out? and now, its better, like 50:50 or something. as for tumor volume I dont know, but, large. and both sides.
Stuff like yours gets me excited. Once again, here we see the heterogeneity of the PCa disease. Street, in your case, I’m guessing that your stellar 0.01 two years after surgery shifts the distribution a good bit (maybe massively) in your favor (certainly as far as GS9 svi ece folks go)!
I’ve always hoped the CARPA-S model was crap (even though I know it’s not), mainly because I was a PSA 37 from the start so that alone gave me mucho points, with nothing else that alarming. Like you, I have a very low (sub 0.006 PSA) a year post surgery, so I’m hopeful the distribution has shifted for me as well. Time will tell. Another uPSA test coming up this week.
I’ve seen one study (link below) where if the participants made it for three years with a sub 0.03 PSA then they had a 90+% chance of making it 7 years without BCR. Roughly similar odds if they had a detectable (more than 0.03) but stable PSA, or very slowly rising (less than 0.05/year).
I think the main message from this paper, and many others that I’ve come across regarding super low post-surgery PSAs, is that these very low uPSAs carry a lot of weight for no recurrence in the near-term, even though this patient will be nervous as hell for his uPSA test later this week….
Well I hope so. Thinking a bit more about the original paper and unfortunate individuals in the highest risk band I wonder if there were either sufficient numbers included in the worst category to be statistically valid and/or a good distribution between high-high and low-high risk (all still scoring in that black line) to trust that it represents a median experience for the score bracket. Maybe too many were gleason 5+4 (type 5 cells dominant) or too many had positive margins after surgery.
Of course doctors at least in my experience hate talking to high risk patients about odds but I just want to know.
Bud you're the "golden patient" as far as my dealings with PC goes over the last 4 years! Yes, you have a high chance of BCR but the fact you've gone this far at .01 is simply amazing and as the above poster pointed out puts you in the unicorn class as far as nomograms go. As far as Capra goes, I'm not a fan. First red flag for me was sample size. Grouping patients all in one catagory(highest risk) and not separating 8-9-10 etc. Also LNI only being 1 point? LVI I would understand but not LNI...that's 2 points for sure. For you with your excellent post-psa levels I would consider a nomogram that includes months/psa along with adverse features a more accurate tool. That HAS to count for something???
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.