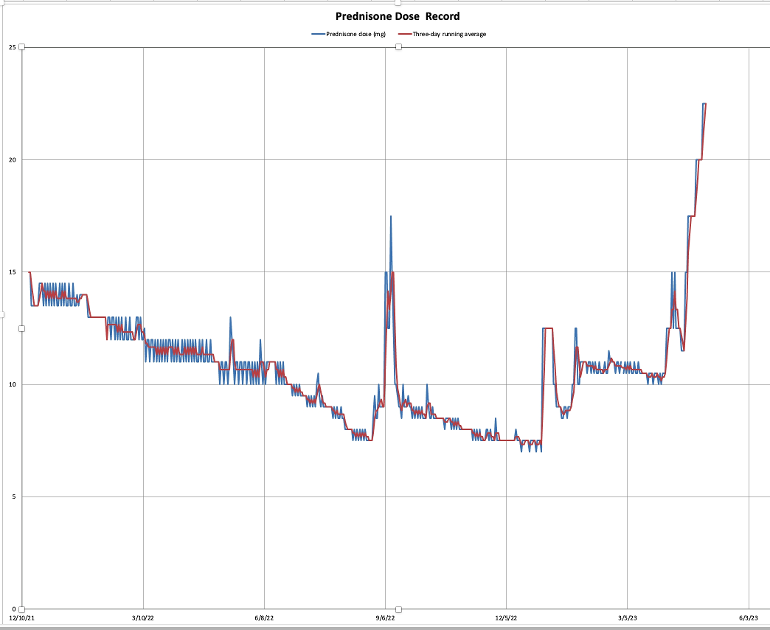
Intial prednisone taper 30 to 8 mg/dy by Aug 2022—then flare
14 months: Successful flare recovery to 7.5 mg/dy by end of 2022-then flare
3 months: Inadequate flare recovery to about11 mg/dy through this March. I did not get above the pain threshold and was tolerating more discomfort (pain and stiffness) trying to limit prednisone exposure—the strategic equivalence of trying to save money by not paying off the credit card account. My motivation for this mistake comes from bone loss (DEXA T-score -2.2 for right femur-neck), and facile muscle injuries I attribute to pred-caused deterioration.
Residual symptoms are:
Pain:
⁃ increasing strongly late evening through 4 AM-ish
⁃ ankles, wrists, upper forearm, lower calf, some shoulders (not the original PMR pains in hips, shoulders, knees);
A lot of stiffness in the knees, elbows, ankles, hips;
Swelling in the knees, calves, ankles, feet.
Lack of exercise energy—I used to run, now walk about 1-hr most days on mild to very hilly terrain.
One month: Through April I have been escalating my pred. dose to “get on top” of the PMR. The problem, and my first and main question is how-the-heck—with the broad range of symptoms—do I figure out where the “top” is.
I will attempt to put a graphical presentation of the taper since the beginning of 2022 at the top of this question.
My dosing strategy is to take the pred about 11–12 PM in enteric capsules (which supposedly don’t release into the small intestine for about 2-hrs) with a glass of yoghurt/milk). The concept is that the prednisone then becomes effective about 4 AM when the cytokines attack. Most recently I have broken off 2.5 mg of the dose taken at dinner to relieve the increase in pain through late evening and night. That seems to have helped. I am now at 22.5 mg/dy the pain is pretty much gone; the stiffness and swelling have decreased by a subjective half.
Question 1: Should I continue increasing the dose to eliminate stiffness and swelling, or declare tactical victory and move into the taper phase.
Question 2: Since I was dwelling at an insufficient 11 mg/dy for three month and have gone so high in my prednisone dose should I start back down at a slow rate (about 1/mg per month) or drop more quickly to where?
Other details: With consultation with my excellent rheumatologist, have just begun weekly tablets of Alendronate (for bone-density stabilization) and monthly infusions of Actrema with hopes the mitigate the need for prednisone. Dietary supplements include Ca, Mg, D3, K2 (and turmeric for good luck). Also omega-3 and an omega-6&3 complex for dry eye. I try to exercise daily (as allowed by body and life). Sleep has improved to mediocre.
I will very much appreciate any help with my questions; the amount of experience, knowledge and responsibility shown by the PMRGCAUK group is amazing.
Written by
JASpmr
To view profiles and participate in discussions please or .
As you have discovered - edging up the dose to deal with a flare really doesn't work well, you are always playing catch-up and allowing inflammation to build up. If you had gone straight to 20mg at the start of the flare. Anyway, now you are there, stay there until you are feeling good, could be a couple of weeks, maybe more. Ony then can you even think about tapering.
The low bone density problem requires a different approach - medication to increase bone density and allow you to remain on the dose of pred you need to manage the PMR symptoms. At best, bisphosphonates only maintain present density and you should have had a dexascan at the intiation of pred to see the status of your bones then. If you want bone density to increase you probably need Prolia or another new generation bone medication to increase density before going back to AA to maintain the improved density (the 2 stages are essential).
The recommendation for tapering is not more than 10% of the current dose at a time and remain at each new dose for 3 weeks to be sure it is still enough, Don't rush, However, once the Actemra starts to work - and that rarely is instant, it can take 3 months or more - then you should be able to taper faster, Actemra is a real game changer - but too many rhemies assume it works immediately and that everyone will get to zero. Neither is true. In the clinical trials half of patients got to zero in a year. Some flared, The other half got stuck at usually 8-10mg due to the fact that GCA has 3 mechanisms causing the inflammation, 2 of them are unaffected by Actemra as biologics are very specific in their action If your disease involves the other two you need pred to manage that inflammation but considerably less. I assume PMR is the same. I have been on Actemra for over a year and have got to 7mg, I struggled to get there and 6mg wasn't possible. It is still a massive improvement on the nearly 20mg I was on this time last year.
It also sounds as if the pred effect on the inflammation isn't lasting the full 24 hours for you. One answer to that is to split the dose and take about 2/3 in the morning and the rest about 2+ hours before you would expect the pain to return. Whether you will need that once the Actemra is working I don't know.
Thank you so much for the detailed answer (even for info I didn't know to ask). I am assuming in your answer that the key to focus on is the pain (which now appears to be in control) and to start downward even with some stiffness remaining. This is the response I was hoping for as I am only too clear about the damages of prednisone and of the damage I've taken in by my taper mistakes.
I will look into Prolia and discuss with my rheumatologist. She is such a good partner that I try to coordinate and communicate with her as I act.
When I moved my pred dose from 20 to 22.5 mg/dy I did that by taking the additional 2.5 mg in the evening, and that seemed to help. I'll try increasing that fraction to the 1/3 range.
You may not need the 2/3 and 1/3 split - just enough later to give 24 hour symptom relief and that will vary from person to person. Don't beat yourself too much - the damage done by pred is often over-hyped and you probably will never get to the accumulated dose I have (WELL north of 50g in 14 years) and everything seems to work fine still, no diabetes, no osteoporosis and it has allowed me to function without much pain or disability for that time.
Thanks again for your support and information. All we can do is our best and get up when we fall down. I included the chart because it illustrates so graphically what happened.
Bone density stabilisation? What does that even mean? What is your t-score?
Sleep, I found, was helped by taking a dose of calcium a little while before bedtime with a small snack. Others have found magnesium seems to have a similar soporific effect.
My DEXA T-score was -2.2 (right-femur neck). I believe the T-score measures mineral density, and by "bone-density stabilization" I meant to keep that density from dropping further.
Thank you for the suggestion on Ca and Mg for sleep. I currently take Ca at breakfast and dinner, but Mg only breakfast. I will try moving the Mg (along with the D3 and K2) to the dinner tranch.
You probably should reconsider whether you should take magnesium and calcium supplements together as calcium tends to be favoured by the body and magnesium might not be so well absorbed. Better to take the magnesium separately.
We do have to take calcium separately from pred (again because calcium can interfere with absorbig pred, and apparently pred also affects the way we metabolise calcium), but I haven't heard the same caveat with magnesium, or other elements, like iron for example.
I do see info on Ca and Mg co-interfering. It adds one more complication to the choreography of supplements/drugs, but can be managed. I'm not seeing information on interference of Ca or Mg with prednisone, but my search on this is not very deep. Where do you see this or other prednisone/supplement interference. My main dose is taken by itself with milk/yoghurt. But now that I've split my pred dose the second part naturally falls into dinner time which includes a handful of supplements.
There is a great deal on the forum about calcium interfering with pred and vice versa. If you take calcium and pred tablets to gether, the calcium is thought to coat the pred tablets before they are absorbed and it slows absorption from the stomach considerably. In the lower gut, higher levels of pred in the blood interfere with the absorption of calcium into the bloodstream. Separating taking the tablets by at least a couple of hours is beneficialm 4 hours is better. Pred for breakfast, calcium for lunch and tea/dinner ...
Thanks. My main dose is well isolated. The second split dose has been taken at dinner with other supplements (Incl. Ca and Mg). I'll have to find a way to separate that split pred dose.
It can be interesting to say the least! When first diagnosed it was found my ferritin was extremely low so I had to take iron supplements. So pred has to be taken separately from calcium. Also iron and calcium don't get along. Thankfully iron and pred ignore each other. But at that time (it is simpler now with reduced doses of everything) I was taking calcium three times a day, pred once, and iron twice. I can't imagine adding a twice a day pred to that mix!
Incidentally, I have read that as long as the magnesium/calcium balance is maintained, calcium is not too much of a bully. It's when we are on increased calcium that it tends to prevent magnesium from being absorbed. I hope/trust that good supplements which include both are designed to help maintain that balance. After all, we do get both magnesium and calcium in a healthy way through food, notably leafy greens. Magnesium is to plants what iron is to animals.
Depends on the medication - and yes, you can improve bone density with supplements and targeted exercise BUT that does require a degree of mobility some don't have.
I did not realize that. JASpmr 's profile indicates osteopenia, and difficulty with exercise because of pain. You must be aware of more context than I have. With the context I'm aware of I'd have thought physiotherapy would be an idea to try before resorting to denosumab.
Just a note to say that prolia/denusomab has to be taken long term because bone density is compromised if you stop. My mum was on denusomab and was fine - lived to 99 and never had a fracture despite numorous falls - but you would need to question a doc whether it is the right med for your diagnosis. A proper doc - my GP didn't know this about dmab. I found out on the forum. Luckily had only had one dose.
But I also have to add that the way it should be used is to increase bone density very effectively and then you can awitch to a bisphosphonate to maintain the level of bone density achieved,
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")