I first had problems with neurogenic bladder 15 years ago but since using daily self-catheterisation apart from initial UTI problems which resolved when I kept 25(OH)D above 125nmol/l 50ng/ml, it's been no problem at all, however that was 15 years ago and for the past year I've had problems which affect sleep duration and quality. Xerosomia (dry mouth) and Reynoulds (cold feet/hands) soles of feet numbness/tingling toes painful ankles that may be related to peripheral neuropathy.
If anyone else if experiencing similar problems it may be because your doctors are not using the most accurate test for those with NEUROGENIC BLADDER to identify
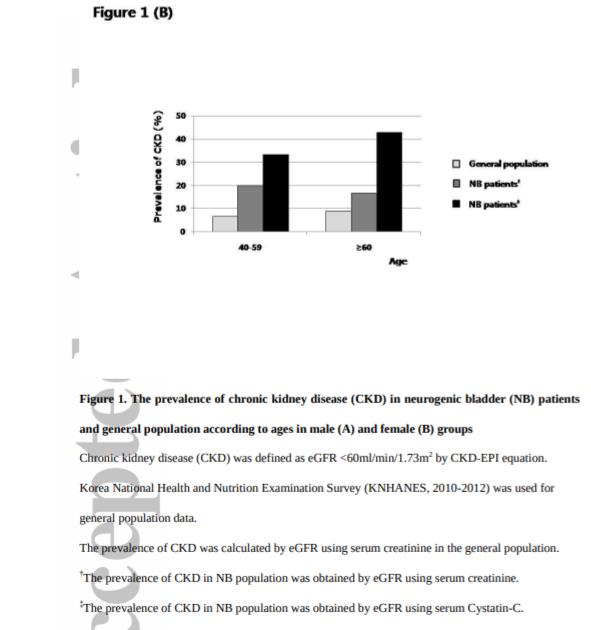
Chronic Kidney Disease in Neurogenic Bladder
AIM: It was believed that neurogenic bladder (NB) might be a risk factor of chronic kidney disease (CKD). However, data are limited regarding the real incidence or risk of CKD in NB. In addition, serum creatinine (sCr), a classical marker of renal function, is not reliable in NB patients because they present muscle wasting due to disuse or denervation. The aim of the study was to estimate the prevalence of CKD in NB patients using serum Cystatin-C. Secondly, we aimed to identify the risk factors for CKD development in NB.
METHODS: This was a cross-sectional study in a public hospital, a specialized center for patients who were victims of industrial accidents. Serum Cystatin-C was checked at the regular laboratory test in the structured NB programme of the hospital, and 313 patients were included in the study.
RESULTS: The overall prevalence of CKD, defined as estimated glomerular filtration rate (eGFR) <60/mL per 1.73m2 was 8.0% and 22.4%, by sCr-based and Cystain-C-based eGFR, respectively, and was greater than age-matched general population in Korea. sCr was not able to detect the early deterioration of renal function in NB patients. Co-morbid diabetes, small bladder volume, recurrent urinary tract infection, and proteinuria were significantly associated with CKD in the multivariable analysis.
CONCLUSION: Chronic kidney disease prevalence was more than three times higher in NB patients than in the general population despite recent progress in the medical care of NB. Co-morbid diabetes, small bladder volume, recurrent urinary tract infection, and proteinuria seem to be the risk factors for CKD development in NB.
The full text downloads from sci-hub in UK however if Sci-hub is blocked where you live message me.
I think most people will not be surprised that people who have lost normal bladder function are going to be more likely to develop kidney problems as they age.
It's unfortunate the test most commonly used to diagnose CKD is estimated glomerular filtration rate (eGFR) <60/ml/1.73m2 which detects far fewer cases of CKD in Neurogenic bladder patients compared to serum Cystain-C-based eGFR which detects far more CKD incidence particularly in patients over 70 yrs old.
You may well have problems convincing your GP the test they are using to diagnose CKD in relation to the symptoms you are describing related to peripheral neuropathy (either diabetic or CKD neurophathy) may not be accurate and serum Cystatin-C may be worth measuring.
