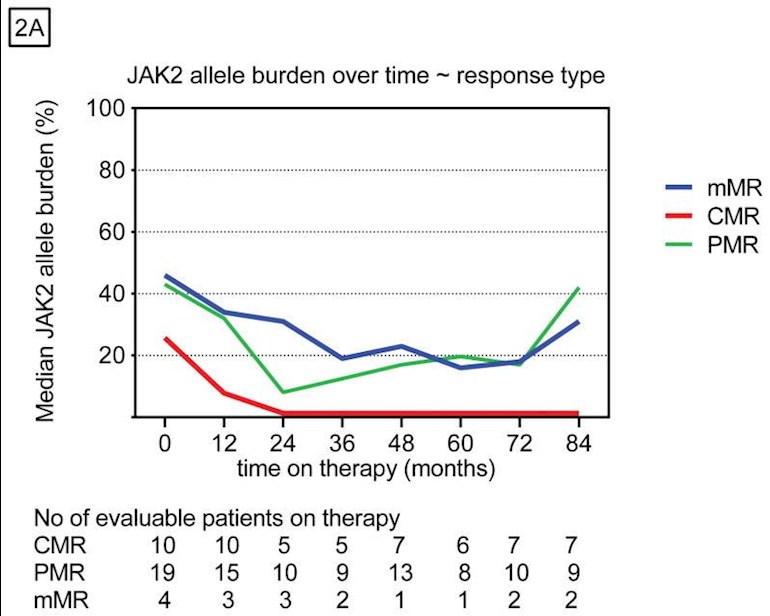
In this report for PEG it tracks for up to 7 years. One trend was apparent:
<<On the other hand, a very important clinical observation is that patients who achieved a CMR (our level of detectability) derived the longest clinical benefit. It remains to be determined whether deeper molecular responses really translate into better clinical outcome compared with patients that only maintain hematologic control. The fact that patients who achieved a CMR did not experience disease progression may support this hypothesis.>>
It means the patients on the red line in this image were least likely to progress. The green and blue partial allele reductions (PMR) had a lower progression benefit with these allele levels reverting upward after 5 years, unlike CMR. 5 years is the current limit of the Ropeg ContiPV study, so seeing any longer results there will be interesting whether any MR is lost.
See next posts here for more images from this study.
Written by
EPguy
To view profiles and participate in discussions please or .
For PV, the results in this PEG study are quite similar to the separate study: ContiPV for Ropeg. (see post #3), suggesting Besremi and PEG are similar in this aspect
From the this study, ET does not benefit on MR (allele or molecular response) from PEG, see red line here. If the current ET trial for Ropeg (Besremi) has a better MR it will suggest a superior action vs PEG, but could instead be the same as here meaning MR via INF is not a good route for ET. There may be other reports with different results on this.
Interesting note, the two alleles converge at 7 years, so maybe there is a predetermined very long term average value for either MPN using INF.
In the study, PV had 20% CMR, ET was 9%, these relating to the red line in the 1st image above. This is ani-intuitive since starting at a lower allele value would seem to give an advantage to the ending allele value.
Compare the lowest dark blue line here (Besremi Allele for PV) to that for PV vs PEG, blue line, above in post #2. Quite similar suggesting equivalent allele action for PEG and Besremi against PV. If the similarity holds, Besremi will lose some benefit and rise after the 5th year here.
Thanks for posting. More food for thought and as you say, is what is the relationship between molecular response, haematological response and 'better outcomes'.
Thanks for this information. From these results it seems the effects of PEG and Besremi are similar for most people - they are both interferons so I guess that's not surprising. Another factor is the side effects of PEG and Besremi. I get terrible fatigue on PEG hence would like to try Besremi which reportedly has less side effects. But as it's much more expensive, if the results are similar, funders will not want to prioritise Besremi. another point: If the effect of interferons starts to reduce after about 5- 7 years, I hope there's something else in the wings.
The main feature of Bes is the longer action and thus more even INF levels in the body over time.
Also, less discussed, PEG and Bes use different formulations for INF. I've posted elsewhere on one aspect of that, the alph-2a (PEG) vs -2b(Bes). And the patent covering Bes discusses a large number of different INF formulas. Does it matter? Could be.
In another MPN group, PV reporter, one commenter said they switched from PEG to Bes and resolved some GI issues.
Agree on the 7 years thing, that is new info to me. My belief is some combo with INF will be an improvement.
In the meantime we can take some comfort re INF in the Long Term INF results from the Silver MPN group:
Very interesting study. My doctor casually mentioned at my last visit she wants me to maybe start trying peg interferon. I am post Et MF and I was told my median survival rate is about 7 years. My allele burden 2 and a half years ago was 63%. So my understanding from the study is the peg interferon probably wouldn’t do much good for me. I consider myself still pretty young, (I’ll be 66 in a couple of weeks), so I was hoping this was better news.
Anyway, I appreciate you posting all this information. The more knowledge one has, the better, in my opinion.
There seems to be INF benefit for MF when it is started early in the MF condition. This includes fibrosis improvements. You could see a reduction in allele also which can't be a bad thing.
For MF, INF and Rux have been trialed together but only Phase 2. This may help if there is INF resistance.
<<combination treatment improved cell counts, reduced bone marrow cellularity and fibrosis, decreased JAK2 V617F burden, and reduced symptom burden with acceptable toxicity in several patients with polycythemia vera or myelofibrosis>>
.
Note the term "several" vs "many". I also don't see the actual data on fibrosis and celluarity.
<<and ten of 13 patients with complete bone marrow response, also achieved MR; seven had CMR.11,29 >>
This matches an association I've been seeing lately in MR, esp CMR, and Marrow remission.
I note that this is dated 2017 and remember that one internationally renowned MPN said at the time that Interferons only had a 5 year window. At roughly this time I was discussing starting Pegasys and managed to consult the two top UK Hems. Both were unconvinced by Dr Silver’s claims that Pegasys was as close to a cure as you can get.
Two years later one of them told me ‘Pegasys is as close to a cure as you can get!’
The other one now much more positive on Pegasys but thinking maybe best to maintain a low dosage even if CMR. (Some pro Peg Hems are saying that if you can keep your JAK2 AB below 10% for a couple of years then can pause Pegasys)
So a lot of new data since 2017 and hopefully positive for those of us dreaming that Pegasys will buy us enough time for a new game changing drug/combo.
Also, I think old statistics must be treated with caution since the participants may be higher risk. Most hems only prescribe Interferons after venesections and/or HU not worked.
Dr Silver’s data set is most interesting because he used Interferons early as a first line.
I agree about the 2017 date. I tend to seek reports with that arbitrary cutoff date, as the field is changing too fast.
That's neat to hear of two experts becoming "INF converts". All of us of course are heavily biased to hear good news, the experts can be a reality check. But they also need to keep up with new info.
<<The reduction in the JAK2V617F allele burden in response to interferon-α-2a (Pegasys) seems more pronounced than that of PegIntron (for the p-values per visit, see the figure).>>
From the same report is this chart. What we and the Drs are excited about are the good responders, in recent posts we've discussed the possible correlation to marrow responses in these. I've seen a consistent pattern that good responses are mostly known by 2 years, as seen here also.
But the poor responders here get no benefit from higher dosage. If all were good responders INF could be all we'd need. Hence the studies on response, where non-driver mutations are one factor.
This contrast in response is a complication that muddles the INF magic.
--
Other reports that may be positively influencing the experts are discussed in Long term INF results, from the Silver MPN Group:
My Dr discounted this because it's a retrospective. But I just realized today, many of the Covid studies are also retro, but these are not discounted in such a way for example today's news:
Thank you for sharing this information on interferon therapy in MPN patients. This is the first time I am reading an article indicating that allele burdens decreased during the first 24 months of interferon therapy, but subsequently increased over time for most of patients in the study. Gives me pause on starting interferon at this stage of my ET to see what other types of combination therapies will be available to increase the likelihood of long-term CMR in ET and PV patients.
I agree, I had not seen that post-5 year result before, although this report has been around for a while.
From this and other shorter studies it looks like INF response is somewhat bifurcated between high and other than high responders. And we can often know which one we are in by year 2. Further, increasing dose may be not effective for low responders.
It could be Besremi has a less obvious bifurcation. If we're lucky they will release year 6 allele data for conti-PV at the Euro hematology meeting later this year. However the German Besremi approval, which a member linked here recently, suggested Conti-PV selected high responders for the follow up phase.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.