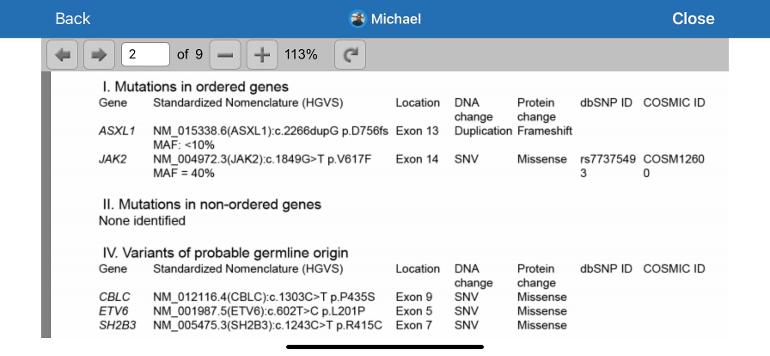
I went back and reviewed my bone marrow biopsy results taken to establish as a baseline prior to Besremi for reference regarding allele burden. There were two mutations present. JAK I already knew about. The other listed is ASCL1. Two questions. Does anyone else have this AS 1 mutation that they know of and if so whether it has any significance?
My second question is does the term MAF 40% for the JAK mean the same thing as allele burden 40%?
Thanks for any info that may be provide.
I have attached the results in question.
Written by
mfh7
To view profiles and participate in discussions please or .
You're correct MAF is same VAF, (variant or mutational allele frequency) or AB (allele burden) all refer to the % of the cell type that is mutated.
To answer your question on ASXL1, it is a significant mutation in some studies, a most recent one found:
"The authors concluded that other mutations notwithstanding, ASXL1 mutations are prognostic of poor outcomes in patients with (Primary) MF but not in those with SMF (post PV or ET MF) "
ASXL1 does not show up in my short search as significant for PV or ET. So it seems to be most associated and studied with Primary MF, but it is worth seeking more info.
The other mutations in your report seem to have not much info for MPN.
This allele burden thing is more of a myth, how relevant is it? Does a low number indicate cure of the disease? Is there anyone who achieves the so-called molecular remission and thereafter never needs any medication for PV?
There is still more focus on hematologic remission, i.e. hct level below 45%, rather than low allele burden. I believe some earlier post has alluded to this.
There is no certain evidence that lowering allele burden (AB) is beneficial. But there are various reports, some discussed on the forum, that lower is better. It's considered most likely to be helpful at the lowest levels (less than 1% for example). But we see here too that some with very high levels are doing fine. As always it's about averages and probabilities.
Until recently this discussion was not even possible, since the only agent that has good odds of large reductions for many is interferon. And only in the last few years has IFN become accepted enough in the clinic to consider the implication.
The 2nd implication is improvements to marrow condition. This can happen separately from AB reduction, or both can happen together.
Regarding a cure, that is currently possible only by marrow transplant (SCT) and that is rarely indicated for ET or PV. What IFN can for some do is called "minimal residual disease (MRD). For example very low AB and/or marrow improvements has enabled some to suspend treatment.
To get AB reductions, this is correlated to hematologic remission (CHR) so if one gets CHR odds of AB reductions are likely improved, but as always there are exceptions both ways.
Some doctor once said, it is important not to over-treat a patient as well as to under-treat a patient. And that is especially true in the case of polycythemia vera.
This is a rare disease, although now classified as blood cancer, yet it was long believed and is still believed not to be life-threatening. What are the excess of red blood cells going to harm the patient, except clogging up the arteries? This is not leukemia in which event the excess white blood cells are attacking the other cells in the body.
MRD or minimum residual disease, is often used in the case of leukemia or lymphoma, where it denotes little or no residue of diseased cells are found if one is lucky enough. Furthermore, the lack of MRD typically means the end of treatment of either chemotherapy or immunotherapy. No more drugs, that is, for the moment until relapse.
Can the same be said about polycythemia vera patients with low or no allele burden? At least, few doctors or patients have made that claim even after many years on interferon or pegylated interferon. Moreover, there is a divine difference between genotype and phenotype. To explain genotype vs. phenotype in the case of BRCA gene mutations, the female carrying one of those mutations is more predisposed to developing breast cancer in her lifetime, but not destined to have breast cancer eventually. Likewise, having a high allele burden of Jak2 mutations does not equate to having a high hemacrit (HCT) ratio, which to some extent would result in clogging the blood vessels and eventually leading to strokes or heart attacks.
There is still no definitive proof of how beneficial a low allele burden is to the patients with polycythemia vera. Currently, the commonly trusted gauge is simply HCT ratio or complete hematologic response. Any claim that a patient should be treated until low or no allele burden is observed may simply be an overkill or a ploy to sell certain expensive medication.
AB and HCT are two different things, HCT is a measure of RBCs in the blood, while AB is a genetic test. Totally different. It is recommended that HCT be below 45, whereas there is no recommendation for AB because it is not nearly as important.
What drug are you using for PV? What are your numbers for AB and HCT now after treatment?
HCT and AB are two different things, but are somehow connected. Indeed, HCT and AB are related to the myeloproferative activity. As you said, a HCT below 45 is recommended . We also know that a JAK2 AB < 50% is also recommended to reduce the risk of thrombosis.
I’m using Pegasys since 2019. My HCT is around 38 for over a year now (67 at diagnosis). My AB is now below 1O%, although I’ll know more precisely at the end of the week.
Interesting point on Leukemia and Lymphoma. Those are caused by, or associated with, various mutations. Do they track only the cell counts, and not mutational burden? That was the practice for MPNs till they discovered the mutations, now most Drs track both.
My view is there is uncertainty currently on allele burden. But I'd like to go for min alleles and find out later it didn't matter rather than not try to reduce it now and find later it would have been useful.
On blood counts vs allele, I have also seen reports of no strong correlations, on average. But there is a pattern that higher alleles, for example Jak2 over 50%, is associated with lower prognosis, and lowering alleles may be beneficial for improved prognosis. There are posts on this area, including a recent one as I recall that had a relation of MF progression to high allele.
Also I've posted a strong relation of CHR to allele reductions on IFN, so I agree there should be no need to way exceed the dose that gives CHR even if allele reduction is a goal. I recently posted on my allele reduction on Bes, I've always had CHR also.
But you're right definitive proof is missing on all of these issues.
Leukemia and lymphoma are considered malignant and life-threatening. For treating these diseases, it is recommended to reach no MRD if possible, for the sake of preventing future relapse. MRD measurement can be conducted with flow cytometry or PCR methods. By some definition, if there is no relapse 5 years after treatment, the patient is considered cancer free or cured, for what it's worth.
PV is generally considered not deadly in most cases. Patients may have 20 years or more of life expectancy after treatment, and for some younger patients it is 30 or 40 years or more. Prognosis is good for this disease. There is more emphasis on preventing blood clots due to the excess of RBCs rather than on disease progression, unless there comes a drug that can cure the patients once and for all, forever not needing to take any medication for PV. Interferon and pegylated interferon thus far have not achieved this. Do you know of any PV patient who stopped taking medication and declared himself or herself cured?
Suggest that you have a detailed discussion with a MPN Specialist about the significance of these results. In addition to JAK2 and ASXL1 there seem to be other findings indicated. I would want to know whether there is significance to these other findings.
It does help to also know the meaning of the types of mutations noted. Here is a bit of information on this. technologynetworks.com/geno...
Genes are supposed to be composed of base pairs abbreviated A-T G-C. How the genes are sequenced determine how they function. The short version is that missense mutations are where mistake in the DNA code and one of the DNA base pairs is changed. Frameshift mutations are where an addition or deletion results in a change in the gene reading frame.
An even simpler explanation is that these genes make proteins. When there is a mutation, it can affect how the proteins are made.
PROTEIN - Missense = PROGEIN
PROTEIN - Deletion = PREIN
PROTEIN - Insertion = PROOOTEIN
This is an oversimplification of a very complex process. Suggest that getting a more detailed explanation from your MPN care team will help you better understand what these results mean. I have also found it helpful to talk to a genetic counselor. You might want to find out if that service is available as well.
Please do let us know what you learn. We can all benefit from your expanded knowledge regarding your results.
Following up on the gene issues after asking my mpn doc about them. He said their is no known significance to the bottom three gene variant findings which were
CBLCETV6
ETV6SH2B3
SH2B3
He said the ASXL1 variant can have significance in some patients in terms of progression but the 10% ASXL1 finding in my instance like has no significance for me in terms of progression or otherwise. I didn’t ask about the JAK positive since we all know what that is.
Separately he is increasing my Besremi dose from 350 mcg to 400 today since hematocrit is above 45 after phlebotomy two months ago and I’m getting a phlebotomy today.
He says it could take a year or more for Besremi to control hematocrit for me. He has some patients where the drug immediately controls hematocrit on small doses and others where it takes a year or more on higher doses and they don’t know why.
I am glad to hear the other genetic variants do not have known issues. My HCT recently jumped up to 47.7 but dropped to 44.4 11 days later (with one 150mcg dose between). We are just holding steady.
I expect response to Besremi and other medications is genetically based. One of the great hopes for the future is treatment based on individual genetic profiles. We are fortunate that knowledge about MPNs is moving forward.
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.