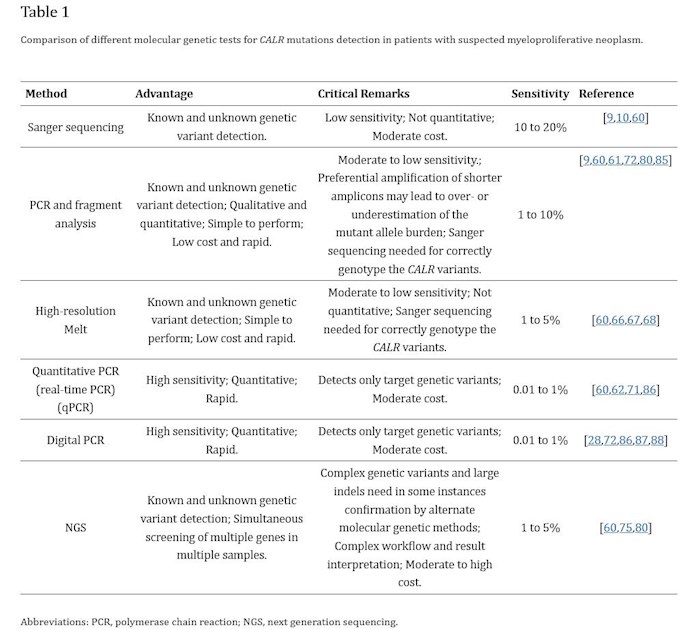
It's come up regularly about whether allele results are accurate and whether the right test was done. I don't offer any answer here, but I came across a table that shows how many different ways there are to test, and the trade offs between them.
This was for CALR but seems relevant to the broad message, that being as always, "it's complicated". But I take it to mean if your results look inconsistent or unexpected, it might relate to which type of test was done.
One thing this shows is NexGen (NGS) is expensive, so this is likely why many MPNs don't have access to this test for large numbers of non-driver mutations.
Written by
EPguy
To view profiles and participate in discussions please or .
Thanks. This report looks at the "what" is measured while the table at top relates to "how" it's measured. Shows how many variables can add up.
But from what I can tell, the report here measured a non-standard parts of the blood on low allele patients (<20% - I am in this range). Platelets and reticulocytes were measured while the standard blood test uses granulocytes. In the image here they found large diffs in AB% with the standard way giving lower results.
This does not seem to address marrow measurements, which probably don't have such variables.
It is a good question whether all of us are getting measured in comparable ways, one hopes it's not an issue.
I think it's not so much a 'what' as it is a 'where' they are looking for VAF. They are looking at the levels in red blood cells, granulocytes, platelets and reticulocytes. I found it interesting as I am of the same description of the patients they discuss - pmf, with no constitutional symptoms, low VAF, and really anemic - I run around 90. My allele burden, or VAF, is under 4%, measured conventionally. It would be interesting to see what the count would be if it was measured in other areas, which the data showed could be much higher. It all, including the info you posted, just goes to show that it is a much more complex an issue it is than just a test with a count as an outcome!
I'm in Canada, so they don't normally report VAF, but it is reported on a Myeloid Panel, Jak2 yes, it was the only mutation other than a trisomy 9, out of 51 tested. My platelets are normally within range, but have been low off and on as a result of the trial drug I am on - Pelabresib, or as it used to be known CPI 0610. I've been on it since July of last year. My most recent (january) bmb showed an improvement in fibrosis of a grade level, and collegen fibrosis dropped from grade 2 to 0, in just 6 months. My blood numbers improved a lot but in the last month have dropped again, which may be due to an increased drug dose. Hopefully they will rebound.
If your collegen grade has dropped from Grade 2 to Grade 0 (a great result) does this mean you are no longer MF? Is your spleen normal size? Your HB is 90? LDH?
I struggle to understand exactly how MF is defined. I’m borderline with a bit of collagen but normal spleen. Makes me MPN-U. My LDH is c. 100. I still appear to be in the proliferative phase but bloods suppressed by low dose Pegasys.
Re my multiple JAK2 tests, the Lab claims 0.2% assay sensitivity.
It doesn't show fibrosis as an endpoint, but I think fibr does not decrease without some sort of treatment. It's double blind, but seems you're likely getting the drug if this is your trial. It's combined with Rux according to this description.
Collegen to zero is quite an accomplishment.
I'm also jak2 15-20% and also had a germline mutation they said is not hematological. NGS brings up everything it seems.
Close! I am in the Manifest 2 trial, which is now closed to new patients, when I started in July 21 I think that was close to the end of acceptances. The big difference between a phase 2 and 3 trial is the primary goal of the 2 is dosage, where as 3 is blind and actual, so with the 3 you could get a placebo. It's a very long trial, I have communicated with people that are entering their 4th year on it.
and the referenced report has this from that post:
<< We consider bone marrow fibrosis improvement to be something that takes a lot of time, so one could imagine that with longer exposure, we are going to see even better bone marrow fibrosis improvement, hopefully of 2 grades or more.>>
No doubt you're familiar with all of these. So fibrosis could continue to improve, while you already got 2 grades better.
Which arm of the Ph2 are you in? Seems they are going for the Rux+ Pelabresib for the pivotal Ph 3 trial.
Hi, I am in Manifest 2, arm 1, transfusion dependent (but I now haven't has one since the 2nd month of the trial). There are 4 arms to the trial, with the newest one being for ET patients being studied in an attempt to reduce platelet levels. My Reticulin FIbrosis only improved a grade level (still a very good thing, and in only 6 months!) It was my collagen fibrosis that dropped to essential 0 from 2. Collagen typically gets worse if the disease has really progressed, so that measure really gave my Hem a thrill (and me too).
The drug is quite well known in the states and Canada now, phase 2 had hundreds of participants - 260 or so, I believe. MPN-NET has had lots of discussion regarding it, and most of the gurus like Mesa have talked extensively about it. It first went into phase 1 trial in 2016, so it is not really brand new or anything, and last fall the company producing it, Cambridge Phara, was sold for a large figure, based mostly on the results of the drug.
Hi Paul; No, I have very serious mf still, my reticulin fibrosis is still Gr 1-2. However it was Grade 2-3 last summer, so a very good drop. My spleen is at the large end of normal. LDH is normal. In Canada we use a different scale for hg, that number would be 9 in the states. I believe the improvement in the last period of months is due to the trial drug, but I am still a candidate for sct, which I am trying to avoid as I do not have a great match - just a 9/10.
Thanks, I’m grade 2 Reticulin fibrosis with focal collagen. My spleen also upper end of normal.
However my HB is c. 140 and I’m not anaemic, my hems say knocking on the MF door but not there yet.
Does this mean you are in the ‘spent’ phase but if your fibrosis is improving, why isn’t your HB rising? And why is your spleen still within normal range.
I assumed that progression would be more obvious? And logical!
Great news that CPI 0610 working so well. Have you tried Pegasys?
Hi Paul, there are quite a few unique forms mf, even pmf. Mine is what is described by my specialist as depletive as opposed to proliferative. In some mf cases, blood cells are simply not over produced at all or are immature still in size etc. It isn't a stage of the disease at all, just a different manifestation. Both my wbc and rbc counts are in the 2's, min normal range is above 4. My platelets normally run close minimum normal, and in fact they ran normal numbers before I was in the trial - pelabresib reduces them, and in fact one arm of the manifest trial is for ET patients as the drug is being studied for platelet reduction. Spleen enlargement is common, but according to the specialists lots of MPN patients, especially those in my category, don't get spleen enlargement, or often any other constitutional symptoms. My HG did rise in the first few months on the trial - I was transfusion dependent in the spring, every 4 weeks. If I didn't have one I could go as low as 70. After I started the trial, I had one more and then no longer required transfusions. That is actually fairly uncommon on the trial. I hit 100 again in December, but since January it has slowly dropped back to around 90 or just under. It may be something as simple as a dosage change though, I will know more within a month on that I suspect. However, according to research, the implication that improved bmf automatically means better disease prognosis is not guaranteed. My specialist says bmb changes are normally slow to occur, and slower to provide tangible results in change. I have not used rux, interferon etc. as my anemia precludes me from them. I did try HU for a while but it was nasty and I think it did damage. I am not an advocate of the current meds due to their side effects and lack of universal disease change, which is why I advocate for the trial drugs. Currently there are 10 mf oriented trial drugs in phase 2 and 3 trials. When I was diagnosed in 2018, there were none. Things are looking up for mpn patients!
Thanks, so when we’re you first dx? And can you please clarify how you progressed?
I simplistically assumed that we go through the proliferative phase, overworking the marrow (causing fibrosis) often thanks to mutant JAK2 and the spleen enlarging (initially to cope with too many rbc and then to help produce more).
So what is the process causing ‘depletive’ MF? Nothing to do with JAK2? What is your spleen not enlarged if low RBC?
People keep saying we are all different but I’ve never come across some as unique as you. I thought I was unusual with LDH of 100 but still progressing.
I was diagnosed in May of 2018, and have always fought anemia and low wbc and rbc counts. They have gradually gotten worse over time, but I have never had even mid range readings. I think the mutation just reacts differently with different situations. Remember, the path between the mutation and the stem cell is conducted by various proteins, and those are the guys that the various BET inhibitor drugs like pelabresib hit - different ones hit different proteins etc. Spleen enlargement is not just related to low rbc as a trigger, and in some cases that trigger never occurs. There are actually a fair number of people like me with mf, although most certainly a minority by a fair bit. The number is enough that we get mentioned any time there is discussion about the need for drugs that go beyond rux etc, as our anemia stops us from using those drugs. Which is why Pelabresib and other trial drugs are so exciting!
I asked my HEM for my allele number and a blood sample was taken during my recent CBC. It was conducted by NEO Genomics. My JAK2 mutation was 56.18% positive. Is this the same number most use to determine how much allele burden we have?
Allele burden (AB) and positive % are the same thing when referring to a specific mutation. (Jak2) But it might get more complex as other mutations are included and each has its own AB.
I got a 5% higher reading from BMB vs blood, (19-14) but usually they are close.
<<allele burden ..is the ratio between mutant and wild type (normal) JAK2 in hematopoietic cells.>>
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.